TECHNIQUES OF RESISTEDEXERCISE
1. STARTING POSITION
• Comfort and stability for the body as a whole.
• Full concentration and force required to overcome the resistance.
2. THE PATTERN OF MOVEMENT
• By passive or free exercise
• Muscle should work in full range.
• Natural pattern of purposeful movement.
3. STABILISATION
• Stabilization of bone of origin improve efficiency.
• Active stabilization provide reinforcement during natural movts.
• If movement at neighboring joints use additional fixation like manual
pressure or strap.
3.
4. TRACTION
• Stretchreflex gives powerful contraction
• Traction throughout range facilitates joint movement and maintain
tension on the muscles.
5. THE RESISTING FORCE
• Variety of means like manual pressure, weights, springs etc
• Pressure exerted on the surface of pt’s skin in the direction of the
movement.
• Manual pressure is adjustable but not measurable
• Mechanical resistance is measurable but not adjustable.
• Maximal resistance elicits maximal response…for power and hypertrophy.
• Sub maximal….more repetitions…endurance.
4.
6. THE CHARACTEROF MOVEMENT
• Smooth, controlled…requiring full attention.
• Speed consistent with optimum rate of contraction for
the particular muscle group.
• Range should be full and resistance and isometric hold
can be applied in any part of range.
7. REPITITION
• Varies according to condition and patient.
• Low resistance-high repetition…more suitable for elderly
and weak pts e.g in O.A.
5.
• HIGH RESISTANCE-LOWREPETITION…disuse after
traumatic injury / orthopedic surgery.
• In joint effusion / pathology like R.A …static
contractions with high repetitions perform in pain-free
range considering fatigue element.
THE CO-OPERATION OF THE PATIENT
• Pt interest is v.imp.
• Can be developed by precise application of resistance,
regular measurement, recording progress, verbal
encouragement and sometimes competition.
6.
RESISTANCES
• Other thangravity and friction
1. THE PHYSIOTHERAPIST
2. THE PATIENT
3. WEIGHTS
4. WEIGHT AND PULLY CIRCUITS
5. SPRING AND OTHER ELASTIC STRUCTURES
6. SUBSTANCES WHICH ARE MALLEABLE(Capable of being
shaped or formed, as by hammering or pressure)
7. WATER
7.
RESISTANCE BY THEPHYSIOTHERAPIST
• Manually by placing hand in direction of movement.
• Stance should prevent wastage of energy and
enable to use body weight and thrusting action of
legs.
• Traction or approximation can be maintained
throughout movt
• Resistance varies according to variation in power
and range
8.
• RESISTANCE BYTHE PATIENT
• Can resist his own movement by sound limb
or by body weight.
• Body weight is also used in free exercise..but
more resistance is applied when muscles work
with reverse origin and insertion.
10.
Progressive resistance exercise
DeLorme’s Progressive Resistance Exercise (PRE) System, which was developed in 1945 as
a method for restoring muscle strength and volume after injury. Here's what it means:
Key Points:
• Origin & Purpose:
• Created by Dr. Thomas De Lorme in 1945.
• Designed for muscle rehabilitation after injury.
• Use of Weights:
• Uses metal weights like barbells or weighted boots to create resistance.
• Determining Resistance (Poundage):
• Based on Repetition Maximum (RM) → The maximum weight a person can lift for a set number
of repetitions.
• Exercise Type:
• Can be dynamic (moving) or static (holding a position).
• Execution:
• Slow and controlled movements to ensure safety and effectiveness.
11.
• Customization:
• Thetraining program varies based on age, temperature, and
the patient’s condition (ensuring safety and adaptability).
• Supervision:
• Clear instructions and proper supervision are necessary to
avoid injury and maximize benefits.
Significance:
• De Lorme’s method laid the foundation for modern
progressive resistance training (PRT), which is widely used
in rehabilitation and sports conditioning. It emphasizes
gradual load progression to safely build strength.
13.
De Lorme AndWatkin
• 10 lifts with ½ 10 R.M
• 10 lifts with 3/4 10 R.M
• 10 lifts with 10 R.M
30 lifts 4 times weekly.
Progress 10 R.M once weekly.
14.
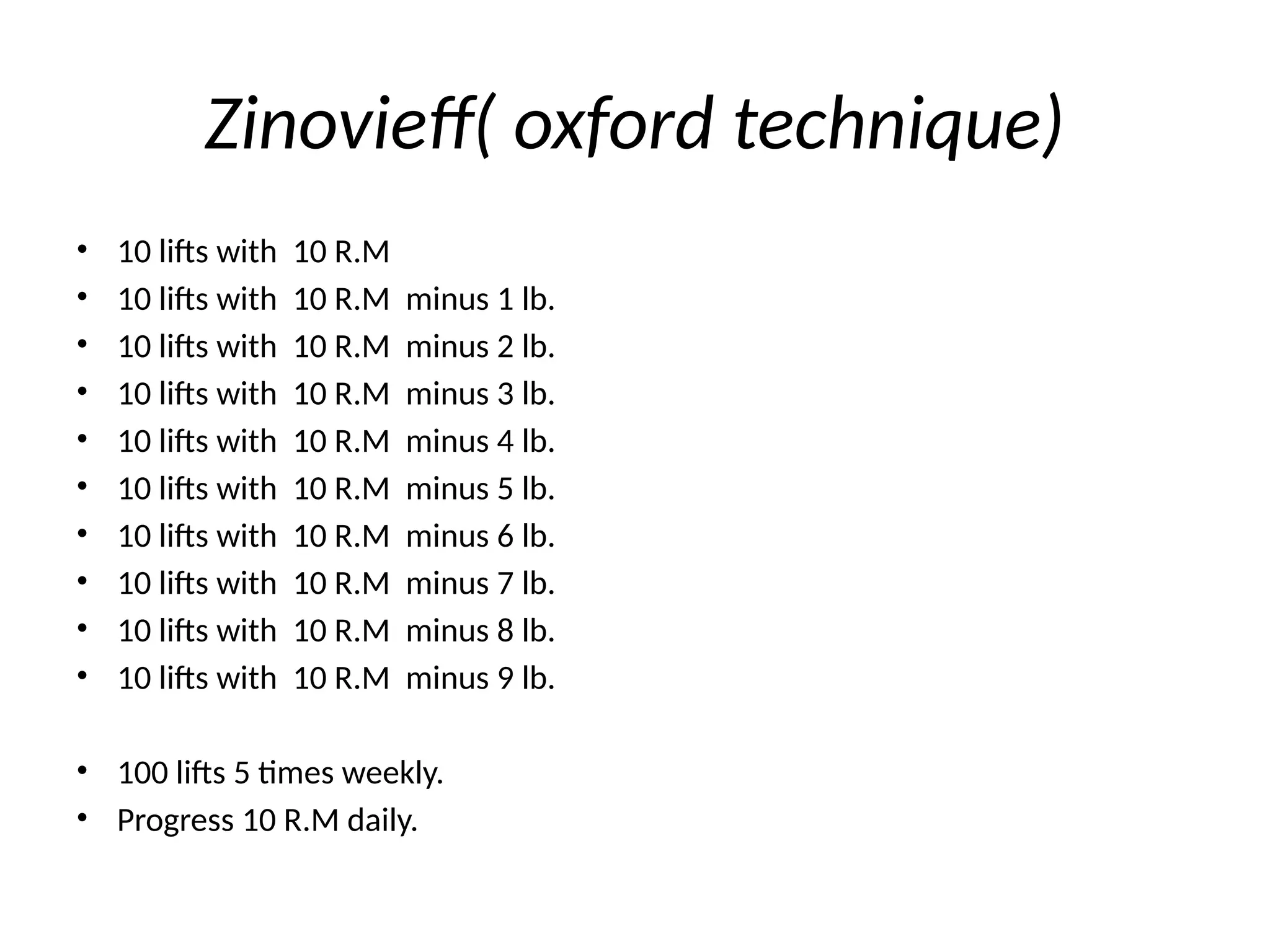
Zinovieff( oxford technique)
•10 lifts with 10 R.M
• 10 lifts with 10 R.M minus 1 lb.
• 10 lifts with 10 R.M minus 2 lb.
• 10 lifts with 10 R.M minus 3 lb.
• 10 lifts with 10 R.M minus 4 lb.
• 10 lifts with 10 R.M minus 5 lb.
• 10 lifts with 10 R.M minus 6 lb.
• 10 lifts with 10 R.M minus 7 lb.
• 10 lifts with 10 R.M minus 8 lb.
• 10 lifts with 10 R.M minus 9 lb.
• 100 lifts 5 times weekly.
• Progress 10 R.M daily.
15.
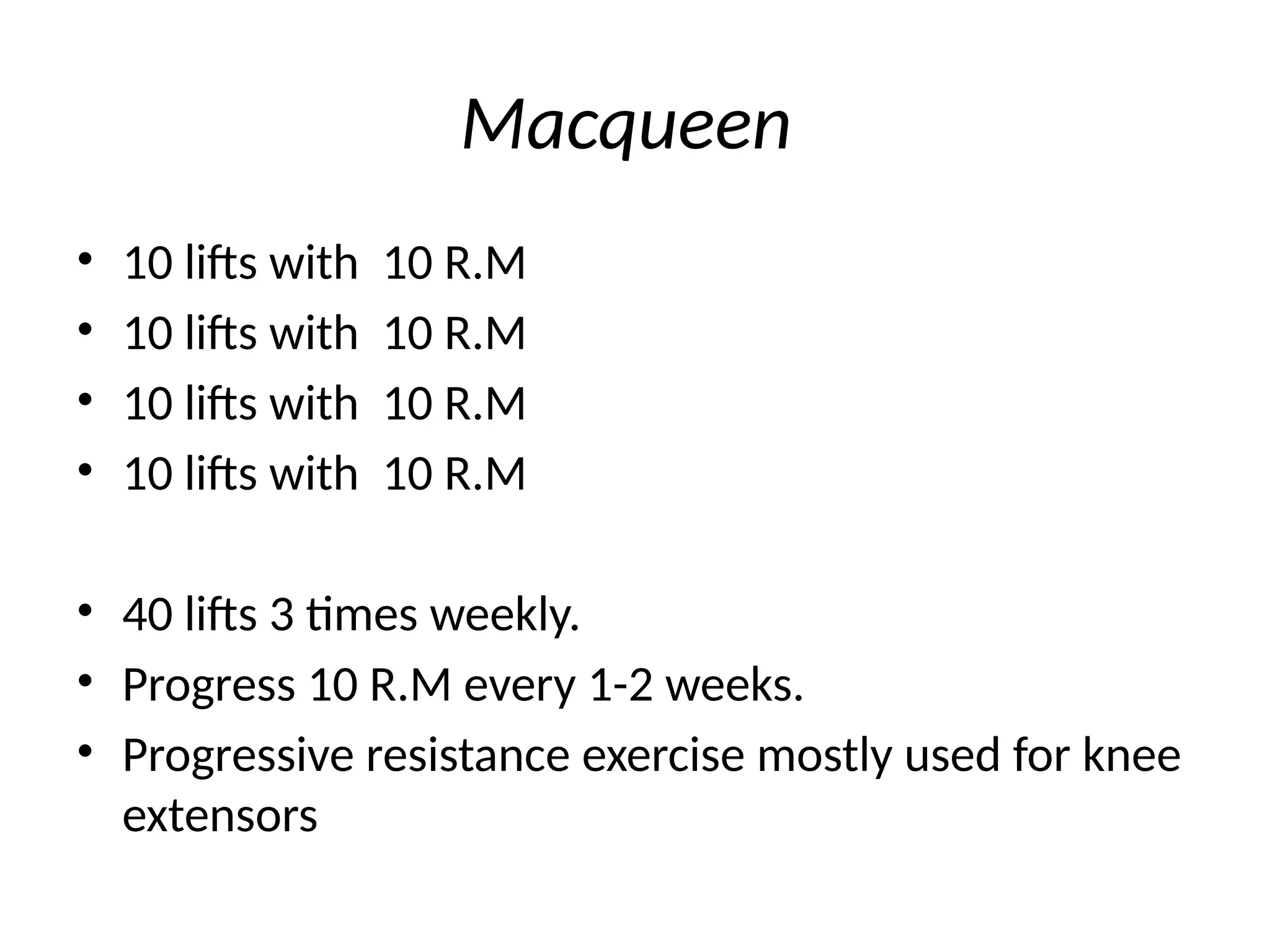
Macqueen
• 10 liftswith 10 R.M
• 10 lifts with 10 R.M
• 10 lifts with 10 R.M
• 10 lifts with 10 R.M
• 40 lifts 3 times weekly.
• Progress 10 R.M every 1-2 weeks.
• Progressive resistance exercise mostly used for knee
extensors























![J._CONTRAST_BATH_THERAPY[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/j-230713132551-5c45004c-thumbnail.jpg?width=640&height=640&fit=bounds)
































































