
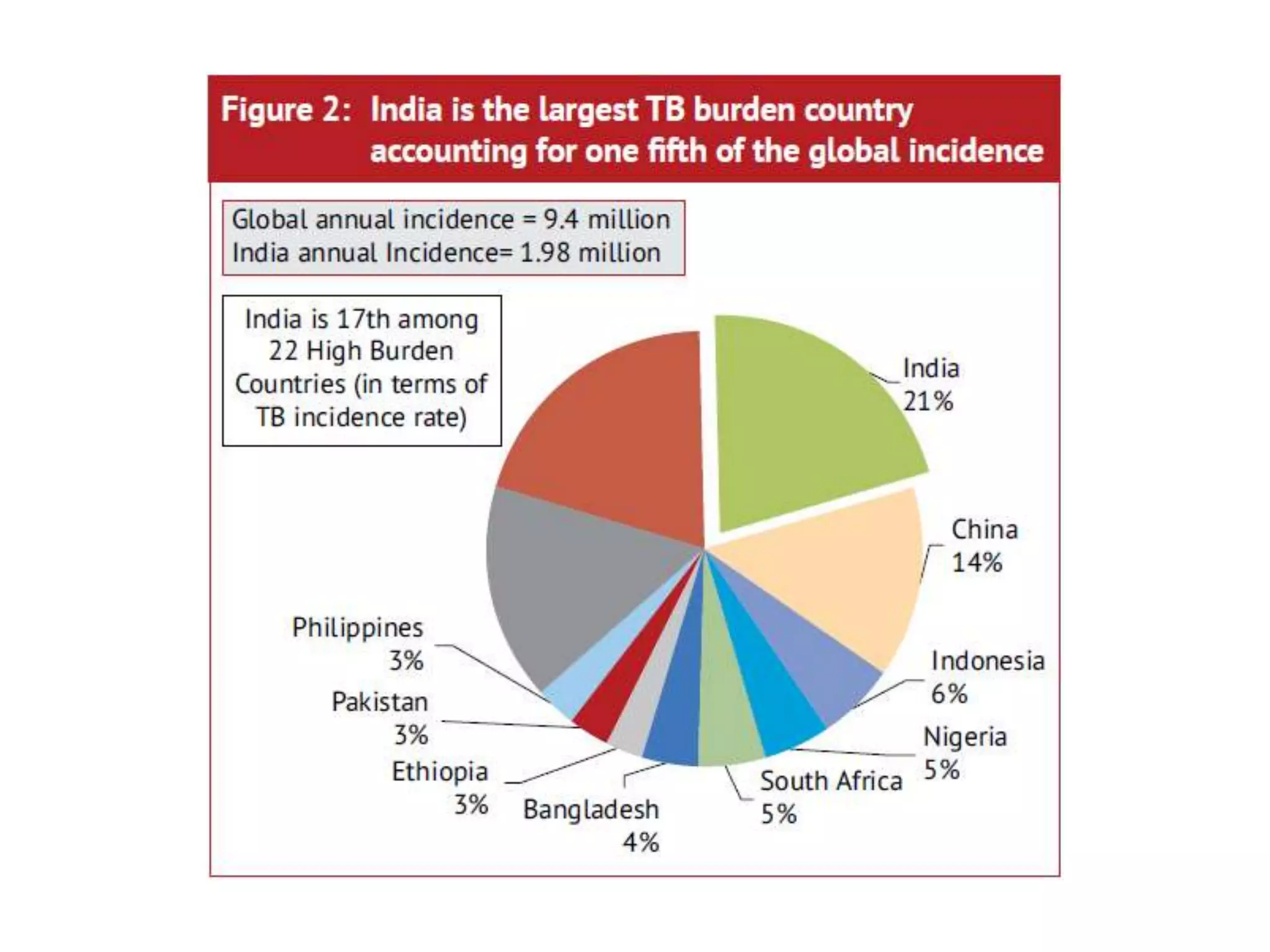
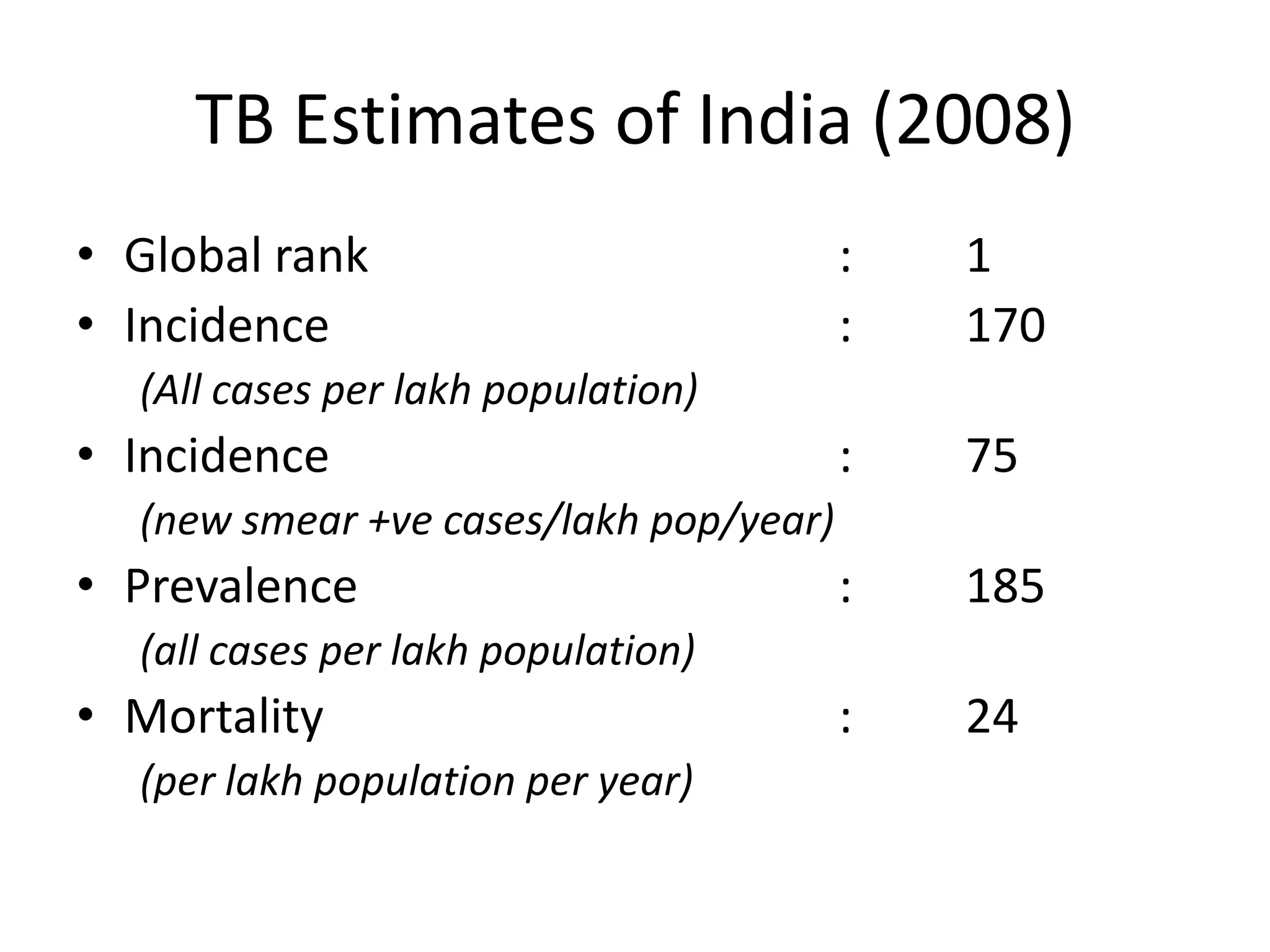
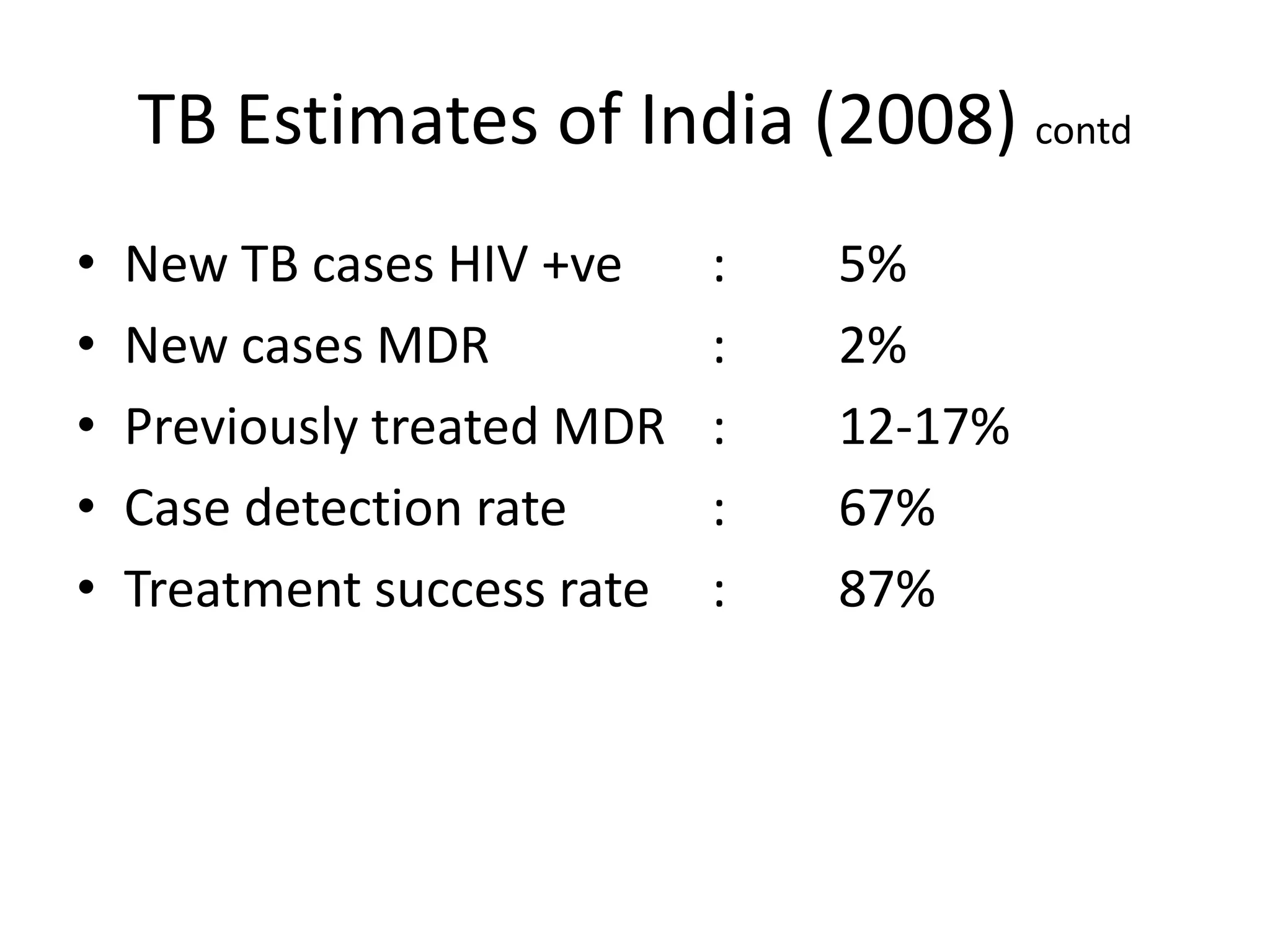
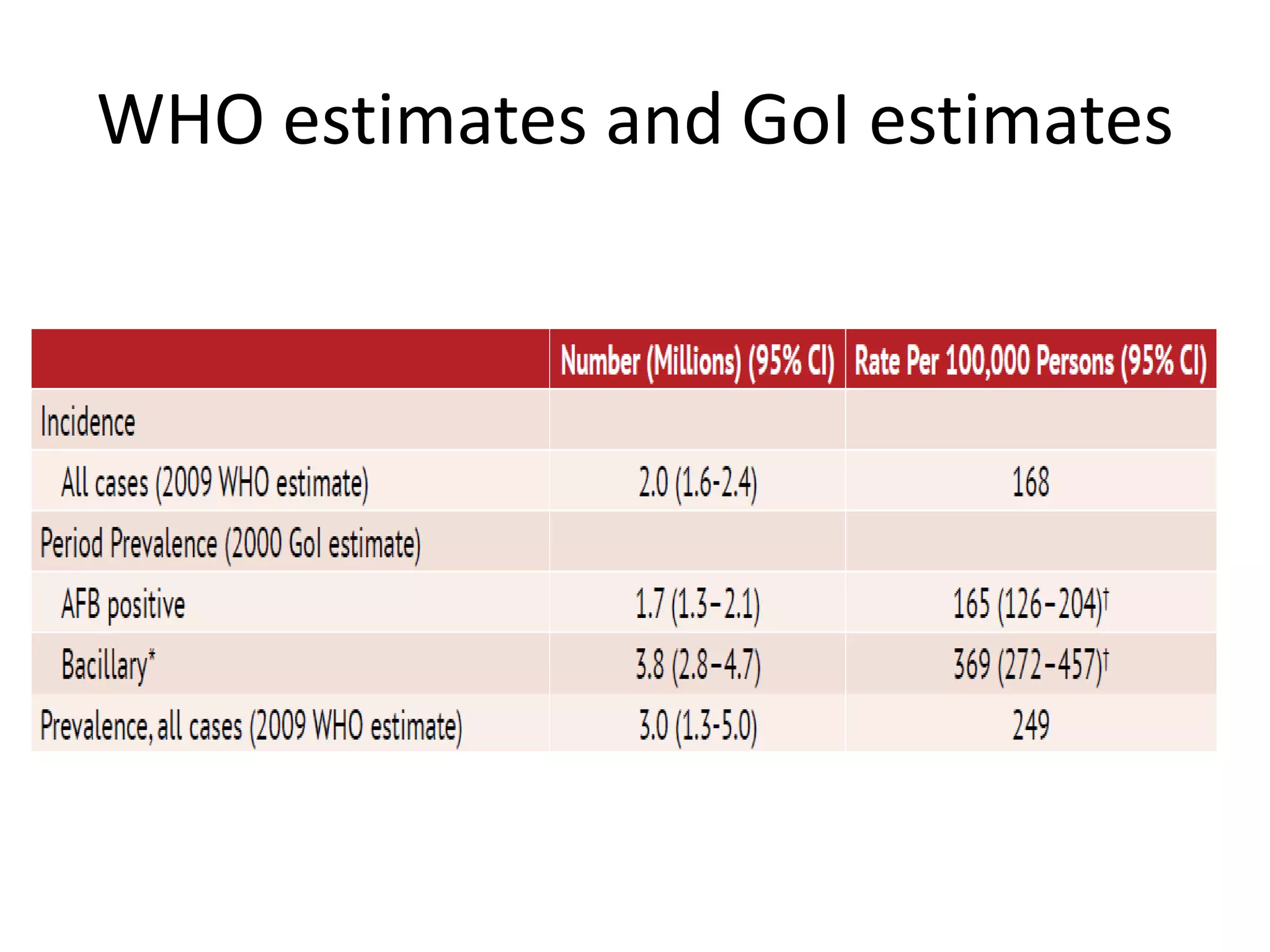
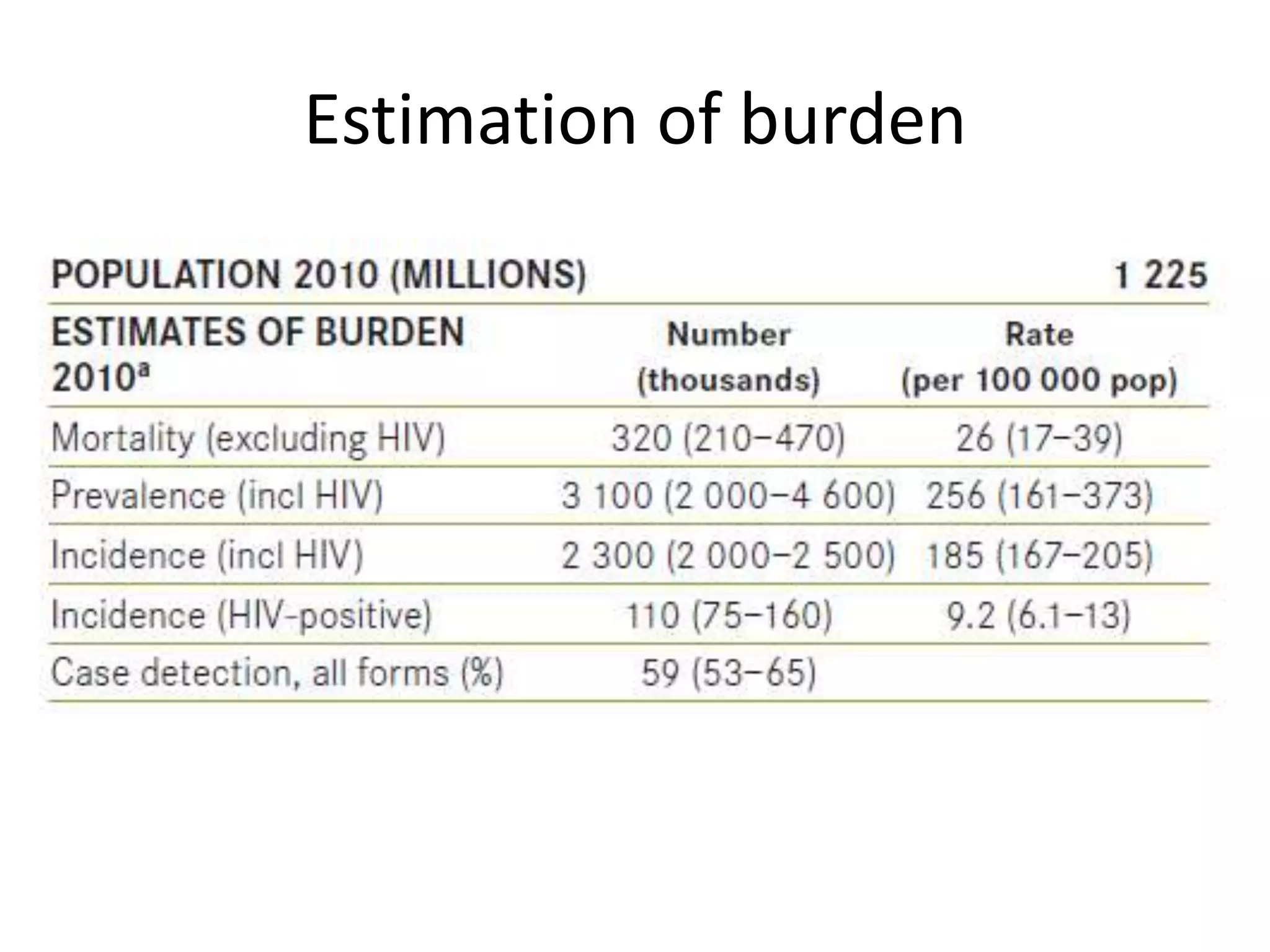
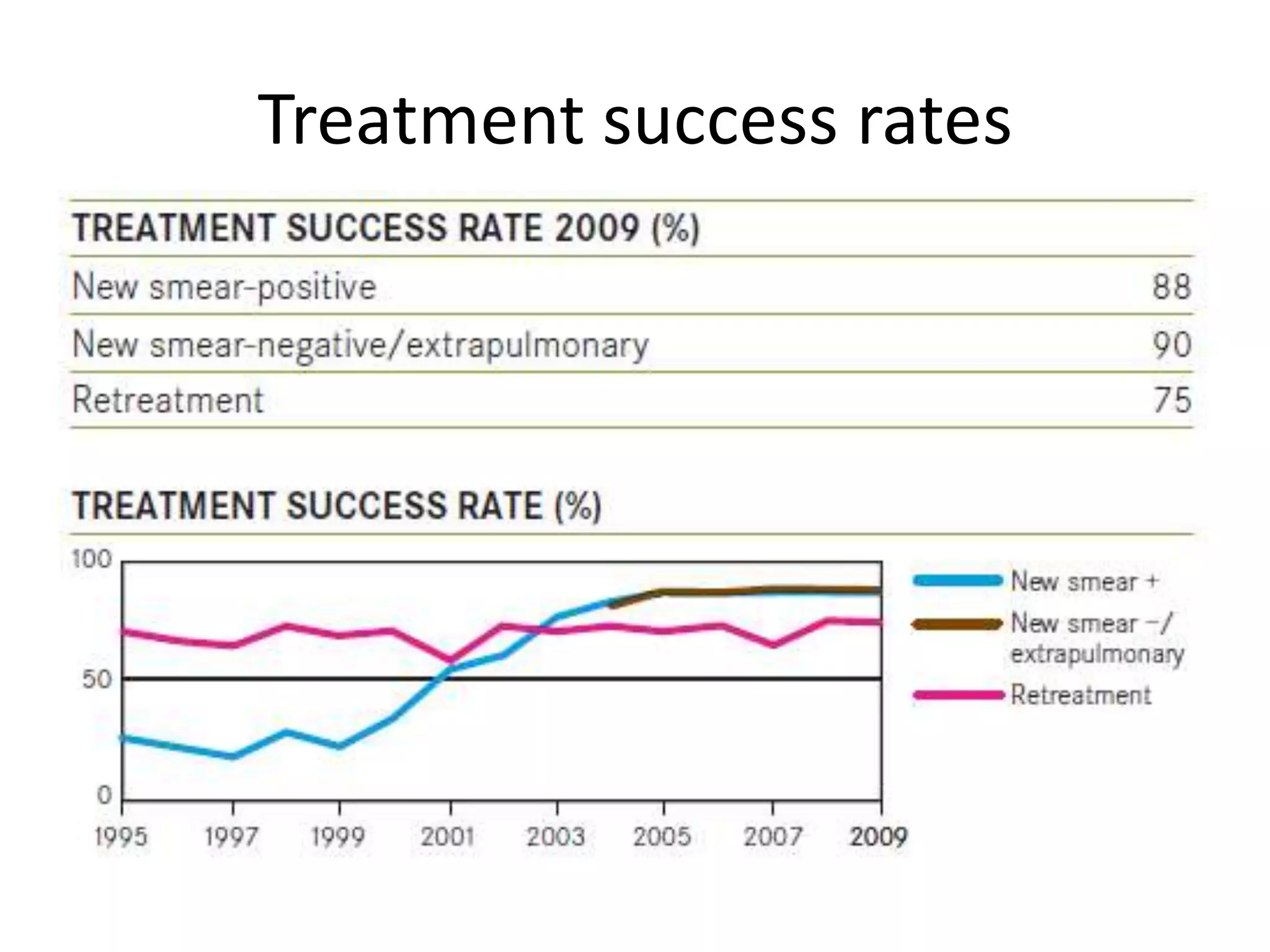
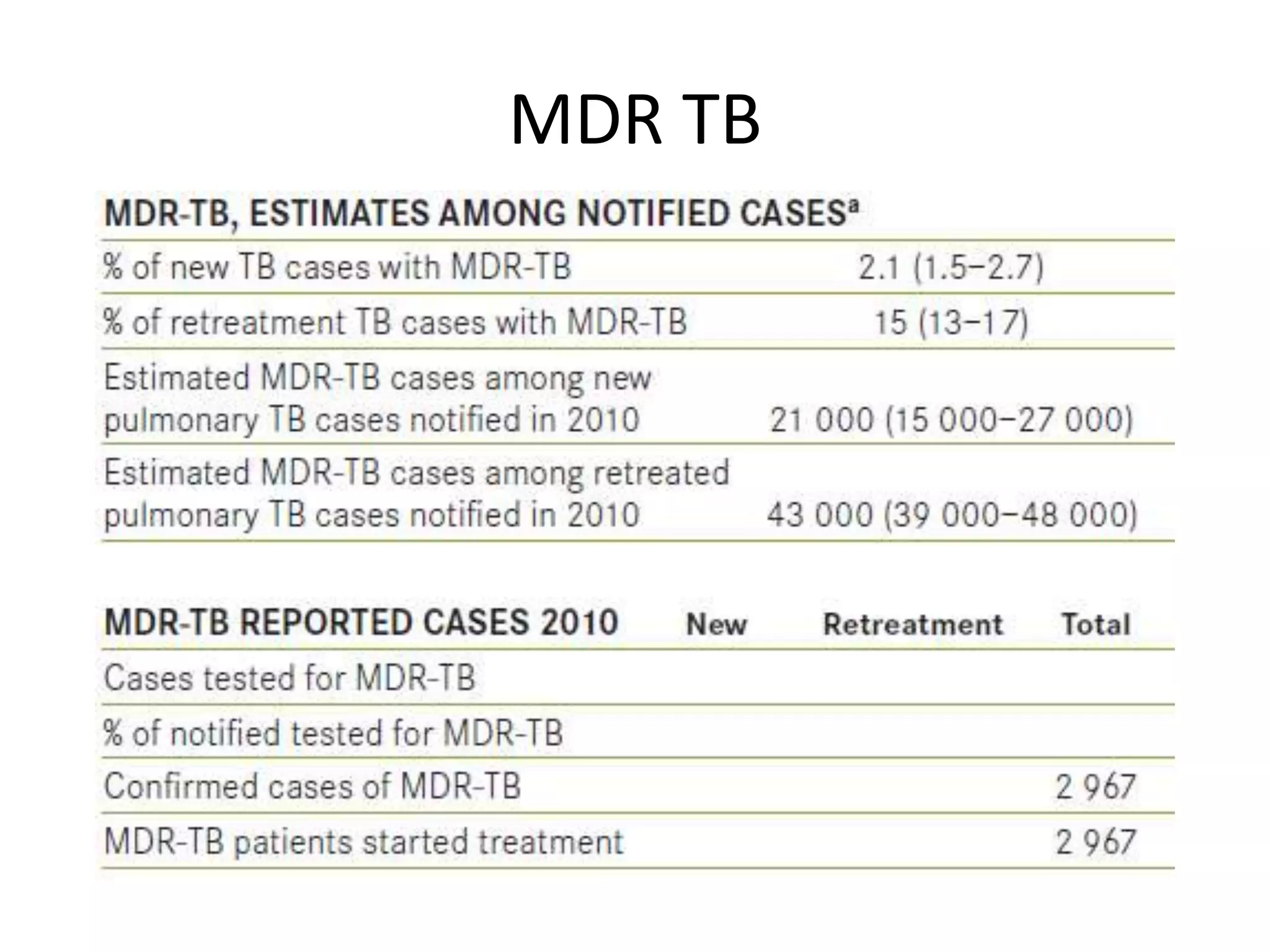
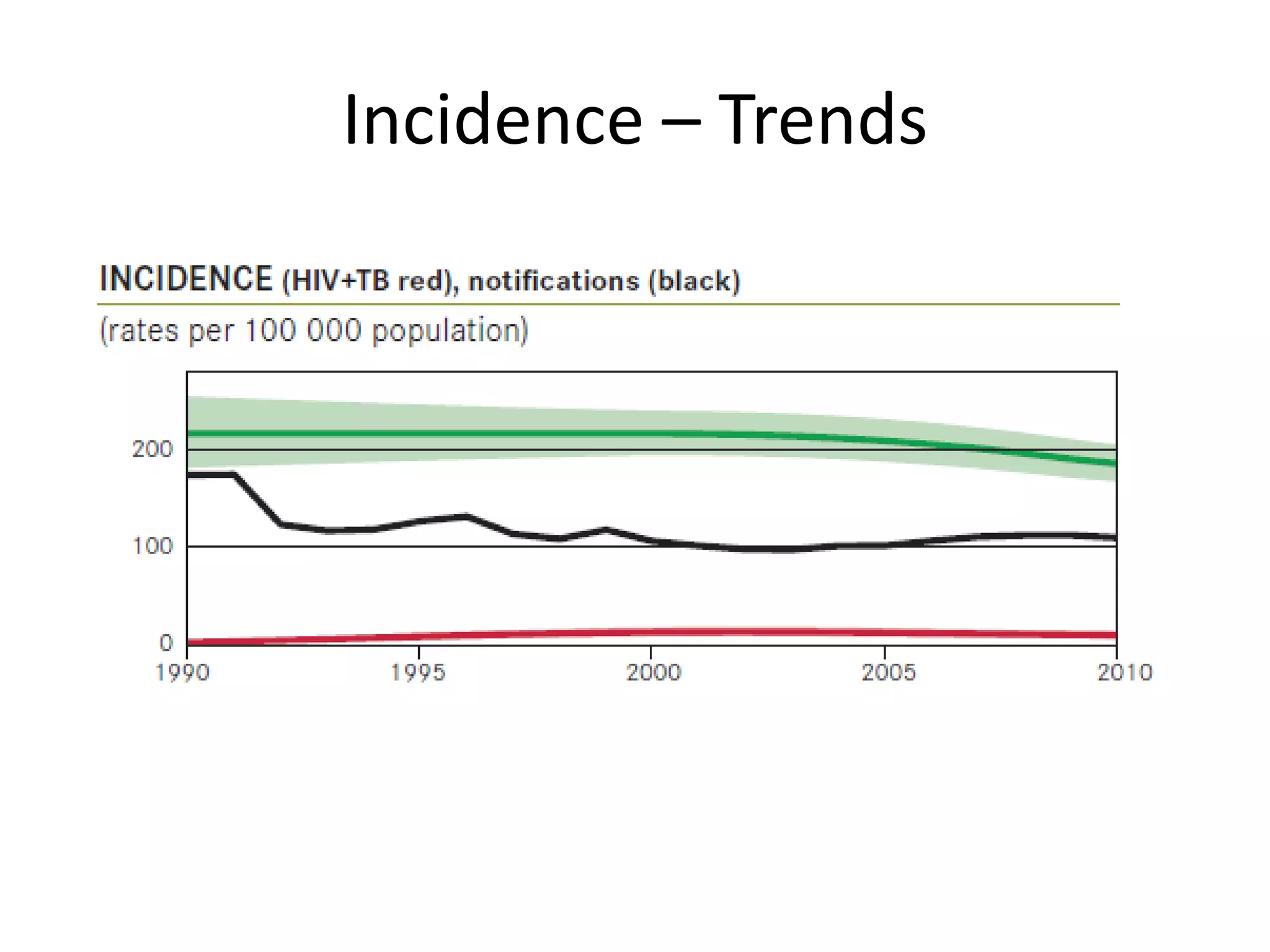
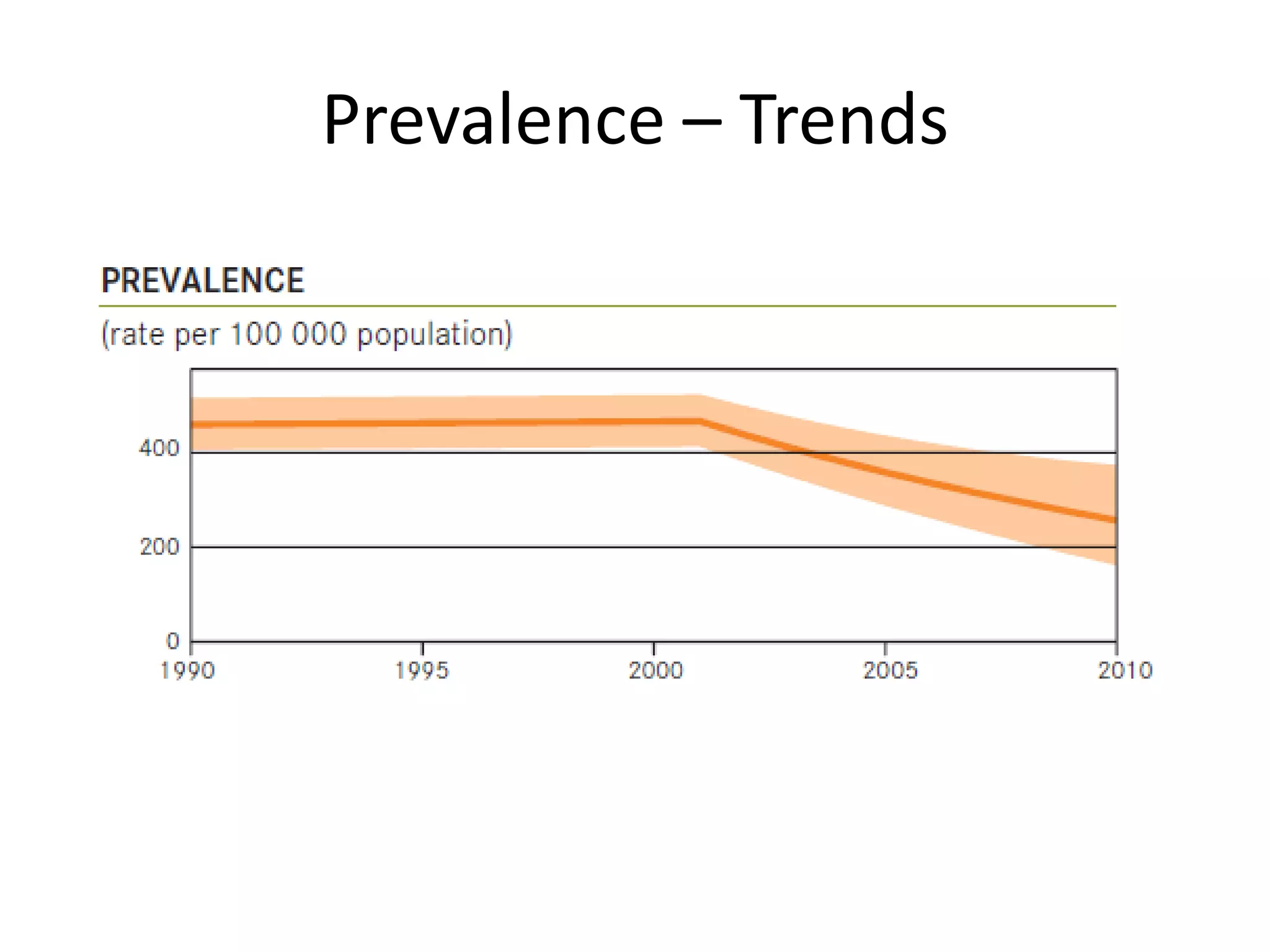
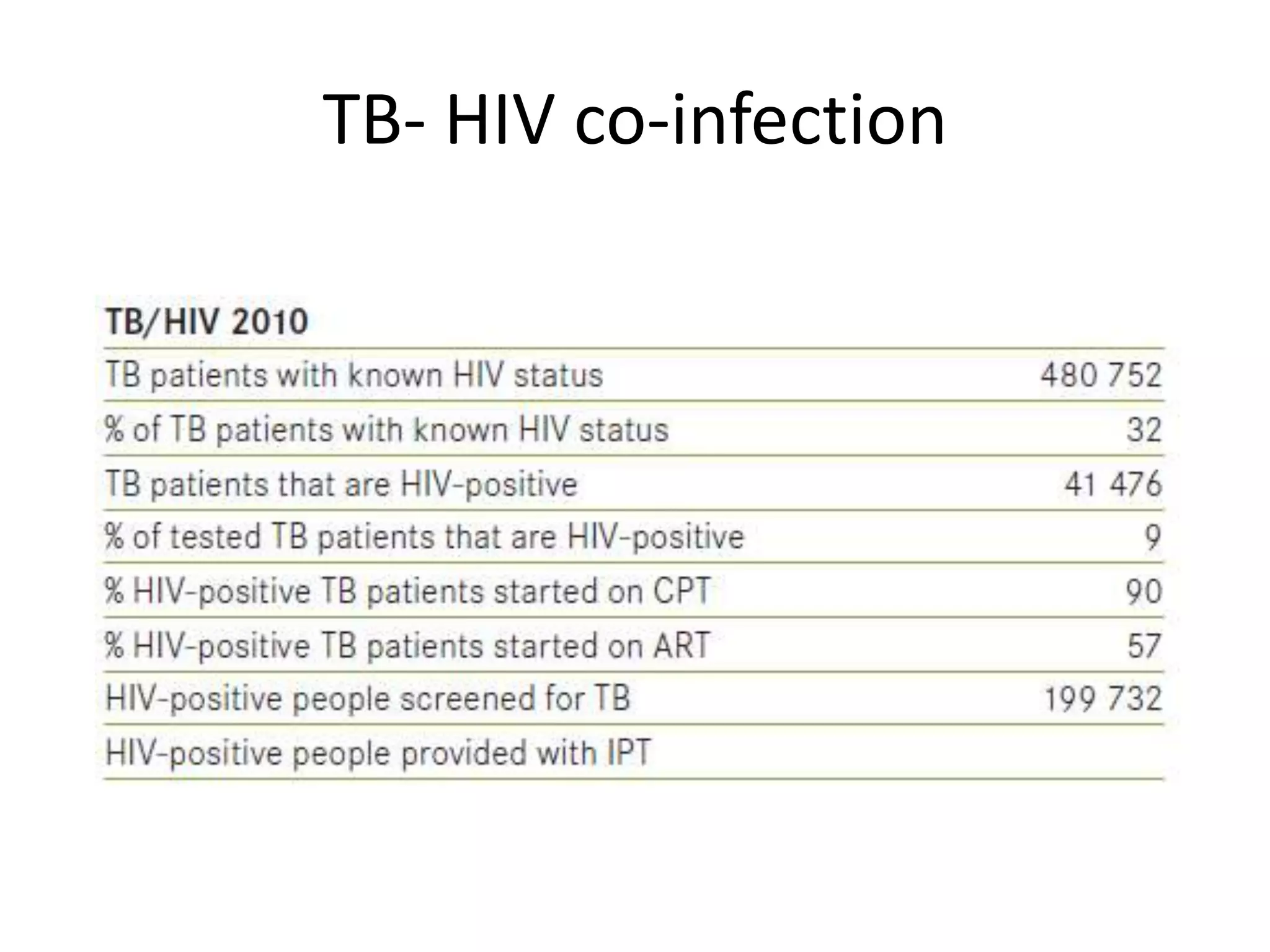


This document discusses tuberculosis (TB) epidemiology in India. It provides background on TB, including that it is caused by Mycobacterium tuberculosis bacteria and primarily affects the lungs. It then summarizes India's high TB burden, with 20% of global cases and high incidence, prevalence, and mortality rates. Key facts presented on India include that it has the world's highest TB burden, an annual risk of infection of 1.5%, and accounts for 66% of the Southeast Asia region's cases. Treatment success rates and trends in incidence, prevalence, and multi-drug resistant TB in India from 2011 are also briefly outlined.




























































![Tuberculosis [Pulmonary] aiims patna mbbs](https://cdn.slidesharecdn.com/ss_thumbnails/tuberculosispulmonary-251109111533-9c0e7eaa-thumbnail.jpg?width=640&height=640&fit=bounds)


























