Downloaded 20 times
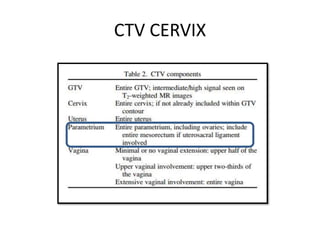
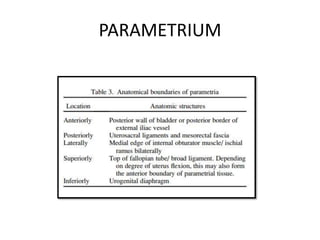

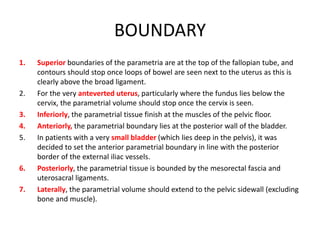
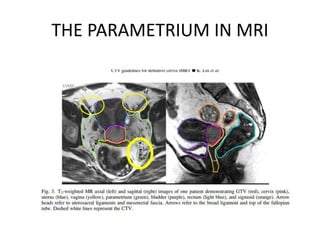
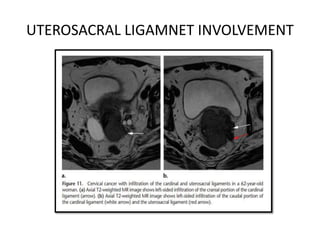
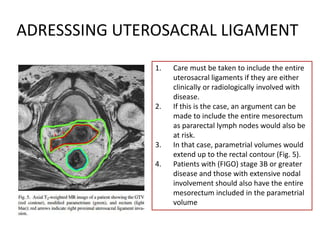
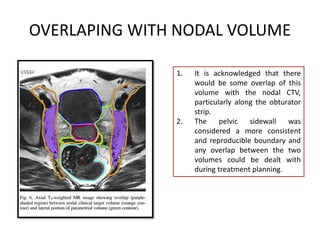

This document provides guidelines for delineating the clinical target volume (CTV) for the parametrium in radiation therapy treatment planning for cervical cancer. It defines the parametrium as the fat and connective tissue surrounding the uterus. The boundaries of the parametrial CTV are described, including superiorly at the top of the fallopian tubes, inferiorly at the pelvic floor muscles, anteriorly at the posterior bladder wall, and posteriorly at the mesorectal fascia and uterosacral ligaments. Special consideration is given to delineation when the uterosacral ligaments are involved with disease based on clinical or radiological findings.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













