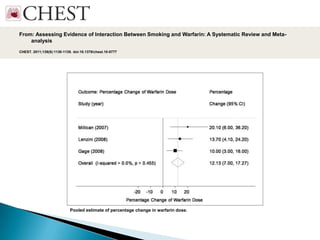
Smoking may potentially interact with warfarin therapy by increasing its clearance and reducing its anticoagulant effects. A systematic review found smoking was associated with a 12.13% increase in warfarin dose requirements and an additional 2.26 mg per week compared to non-smokers. While earlier studies did not find a relationship between smoking and INR levels, recent evidence suggests smoking can significantly impact warfarin therapy through enzyme-inducing effects.



![ RESULTS :
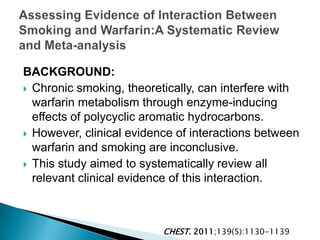
◦ We identified 2,278 cases and 5,927 controls.
◦ Subjects comprised mostly postmenopausal white
women with a mean age of 66 years and a
current smoking prevalence of 10%.
◦ Compared to never-smokers, current and former
smokers were at higher risk of VT (adjusted OR
1.21, [CI] 1.02-1.44 and OR 1.15, CI 1.03-1.29.
◦ These associations were attenuated for
potential mediators (cardiovascular
disease, congestive heart failure, cancer, recent
hospitalisations and physical activity): OR 1.02 CI
(0.83-1.25) and 0.95 CI (0.83-1.08).
Thromb Haemost. 2013 Mar 7;109(5)](https://image.slidesharecdn.com/tabagismeetthrombosehabbal-130527103856-phpapp02/85/Tabagisme-et-thrombose-habbal-26-320.jpg)