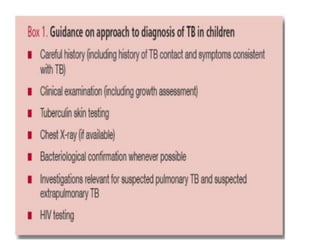
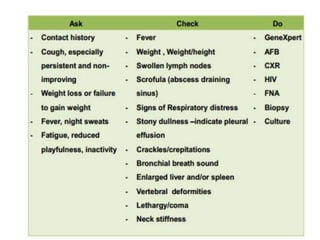
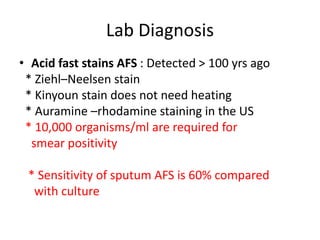
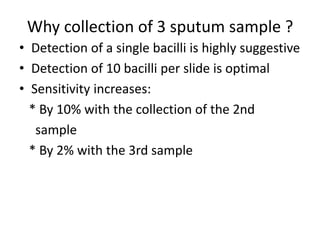
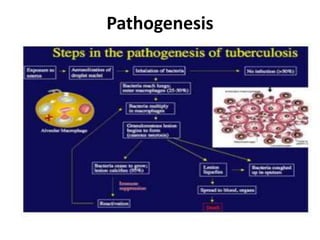
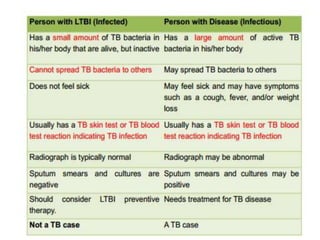
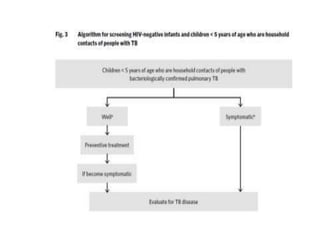
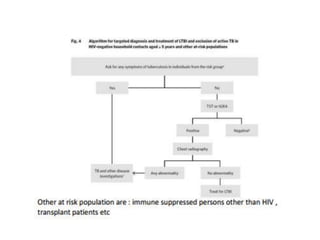
The document provides a comprehensive overview of tuberculosis (TB), including its global prevalence, classification, diagnosis, transmission routes, and treatment. It highlights the significant burden of TB, particularly in high-burden countries like India and Ethiopia, and outlines clinical features and complications associated with pulmonary and extrapulmonary TB. Additionally, it discusses diagnostic methods, including culture and molecular tests, and emphasizes the importance of preventive measures and nutritional support in managing TB, especially in pediatric populations.
















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


