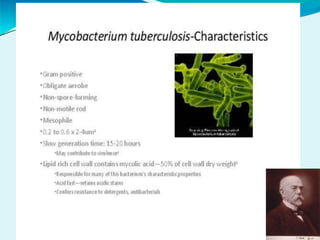
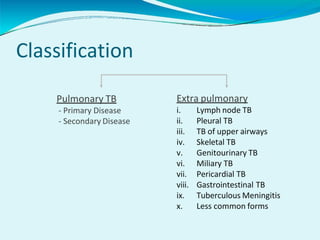
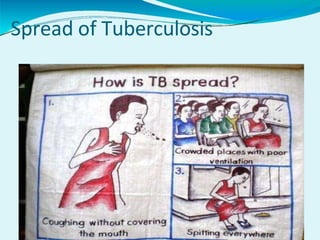
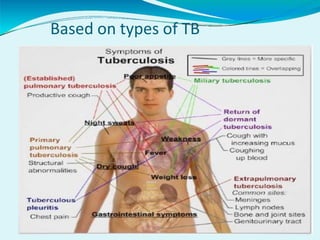
Tuberculosis is an infection caused by Mycobacterium tuberculosis that mainly affects the lungs. It can spread through droplets in the air from coughing or sneezing. Symptoms include persistent cough, chest pain, coughing up blood, fatigue, and fever. TB is classified as pulmonary or extra-pulmonary depending on the affected area. Diagnosis involves sputum tests, chest x-rays, and the tuberculin skin test. Treatment requires a multi-drug regimen over several months. Preventive measures include BCG vaccination, isolation, and proper ventilation. Drug-resistant forms like MDR-TB and XDR-TB are major challenges. Co-infection with HIV increases the risks of TB infection and


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

