Definition of SLE
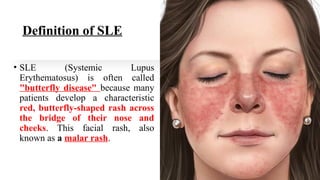
•SLE (Systemic Lupus
Erythematosus) is often called
"butterfly disease" because many
patients develop a characteristic
red, butterfly-shaped rash across
the bridge of their nose and
cheeks. This facial rash, also
known as a malar rash.
5.
Systemic lupus erythematosus(SLE) is a chronic, systemic
autoimmune disease with many manifestations and multisystemic
involvement (multisystem inflammation) that predominantly affects
young women (Approximately 90% of cases of SLE occur in women) and
caused by the immune system attacking its own cells.
Certain ethnic groups are more vulnerable than others to developing
SLE.
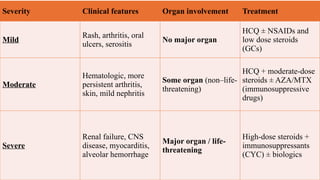
The condition has several phenotypes, with varying clinical
presentations from mild mucocutaneous manifestations (Skin)to
multiorgan and severe central nervous system involvement.
Systemic lupus erythematosus (SLE) is characterized by antibodies to
nuclear and cytoplasmic antigens and a relapsing and remitting course.
8.
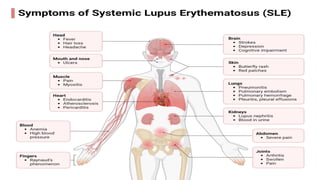
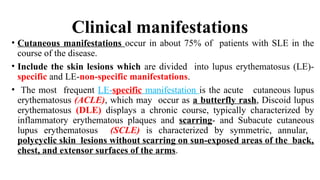
Clinical manifestations
• Cutaneousmanifestations occur in about 75% of patients with SLE in the
course of the disease.
• Include the skin lesions which are divided into lupus erythematosus (LE)-
specific and LE-non-specific manifestations.
• The most frequent LE-specific manifestation is the acute cutaneous lupus
erythematosus (ACLE), which may occur as a butterfly rash, Discoid lupus
erythematosus (DLE) displays a chronic course, typically characterized by
inflammatory erythematous plaques and scarring- and Subacute cutaneous
lupus erythematosus (SCLE) is characterized by symmetric, annular,
polycyclic skin lesions without scarring on sun-exposed areas of the back,
chest, and extensor surfaces of the arms.
9.
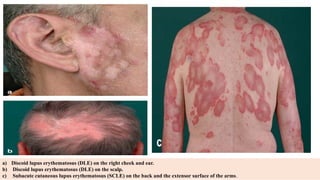
a) Discoid lupuserythematosus (DLE) on the right cheek and ear.
b) Discoid lupus erythematosus (DLE) on the scalp.
c) Subacute cutaneous lupus erythematosus (SCLE) on the back and the extensor surface of the arms.
10.
The LE-non-specific manifestationsinclude the following:
• The musculoskeletal system is involved in around 90% of
patients with SLE. In addition to myalgia and arthralgia,
arthritis of small and large joints may occur.
• SLE may lead to joint deformation.
• About 50% of patients with SLE develop renal involvement.
Lupus nephritis is a glomerular nephritis, typically with
(proteinuria and cellular casts).
• Cardiovascular manifestations of SLE include pleuritis &
myocarditis.
• Pulmonary involvement include lupus pneumonitis and
pulmonary fibrosis are rare.
• The central nervous system is affected in about 15 to 50% of
patients with SLE include seizures.
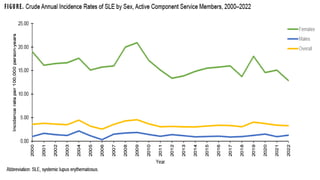
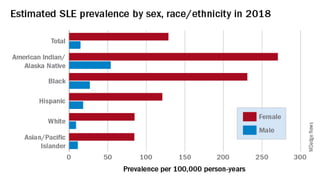
Epidemiology
Prevalence and incidence
•Globally, the reported incidence and prevalence of SLE differ significantly by geography, More common
in certain ethnic groups: African, Asian, and Native American populations have higher prevalence and
more severe disease. Lower prevalence in Europeans. This disparity can be attributed to the
environmental surroundings and genomic differences
Sex
• SLE is more prevalent in the female population more than male.
• Estrogen is thought to contribute to susceptibility.
Age
• Age Peak onset: 15–45 years (reproductive age).
• Can occur in children (juvenile SLE) or older adults (late-onset SLE), but clinical presentation may differ.
Mortality
• People with systemic lupus erythematosus (SLE) have a higher risk of dying compared to people of the
same age and sex in the general population without SLE.
• The most causes of death internationally include infection and cardiovascular disease, which can
probably be mitigated through improved quality of care.
(Mortality has improved due to earlier diagnosis and better therapy)
13.
Notes:
Ethnicity, sex andage play a significant role
in determining the clinical outcome and
management of the disease.
Difference between prevalence and incidence:
Prevalence Definition: The total number of existing cases (both old and new) of a
disease in a population at a specific point in time (point prevalence) Tells you: How
widespread the disease is.
Incidence Definition: The number of new cases of a disease that develop in a population
during a specific period of time. Tells you: The risk of developing the disease.
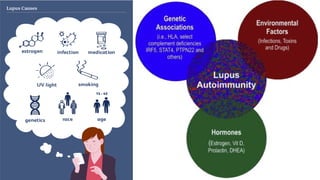
Etiology of SLE
•Theetiology of systemic lupus erythematosus (SLE) is
idiopathic (Unknown) but multifactorial, meaning it
doesn’t come from a single cause but rather from an
interaction of genetic, hormonal, environmental,
and immunological factors.
19.
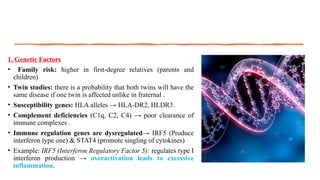
1. Genetic Factors
•Family risk: higher in first-degree relatives (parents and
children)
• Twin studies: there is a probability that both twins will have the
same disease if one twin is affected unlike in fraternal .
• Susceptibility genes: HLA alleles → HLA-DR2, HLDR3.
• Complement deficiencies (C1q, C2, C4) → poor clearance of
immune complexes .
• Immune regulation genes are dysregulated→ IRF5 (Produce
interferon type one) & STAT4 (promote singling of cytokines)
• Example: IRF5 (Interferon Regulatory Factor 5): regulates type I
interferon production → overactivation leads to excessive
inflammation.
20.
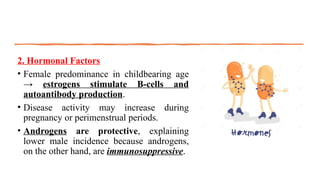
2. Hormonal Factors
•Female predominance in childbearing age
→ estrogens stimulate B-cells and
autoantibody production.
• Disease activity may increase during
pregnancy or perimenstrual periods.
• Androgens are protective, explaining
lower male incidence because androgens,
on the other hand, are immunosuppressive.
21.
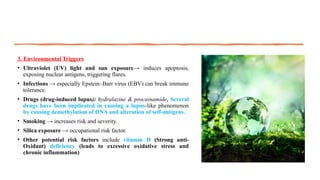
3. Environmental Triggers
•Ultraviolet (UV) light and sun exposure→ induces apoptosis,
exposing nuclear antigens, triggering flares.
• Infections → especially Epstein–Barr virus (EBV) can break immune
tolerance.
• Drugs (drug-induced lupus): hydralazine & procainamide, Several
drugs have been implicated in causing a lupus-like phenomenon
by causing demethylation of DNA and alteration of self-antigens.
• Smoking → increases risk and severity.
• Silica exposure → occupational risk factor.
• Other potential risk factors include vitamin D (Strong anti-
Oxidant) deficiency (leads to excessive oxidative stress and
chronic inflammation)
22.
4. Immunological Factors
•Defective clearance of apoptotic cells → act as self
antigen
• Autoantibodies (ANA, anti-dsDNA, anti-Sm) form
immune complexes.
• Loss of self-tolerance → autoreactive T and B cells
survive.
• Type I interferons (especially IFN-α) are
overproduced → drive chronic immune activation.
• Immune complex deposition → inflammation and
multi-organ damage.
23.
Note:
• Genetic Refersto the DNA sequence itself (the code of your genes).Stable: Inherited from parents and does not change (except by mutation).
• Epigenetic: Refers to changes in gene expression without changing the DNA sequence. Controlled by chemical modifications (like DNA
methylation, histone modification, microRNAs). Reversible and influenced by environment (diet, infections, stress, toxins).
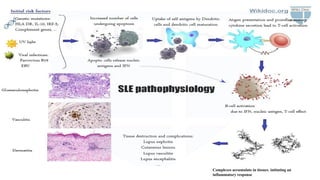
Pathogenesis
of SLE
• Thiscomplex interaction between genetic factors ,
environmental triggers and the collapse of
immunological tolerance results in the
generation of autoantibodies with pathogenic
potential due to exposure of self-antigens to the
immune cells possibly from an increased apoptotic
cell load, initiates interaction between innate and
adaptive immunity.
• Which leads to formation of immune complex
promoting the accumulation of immune
complexes across diverse tissues and organs due
to the deficiency in complement components.
• Such deposition initiates episodes of
inflammation and organ damage.
27.
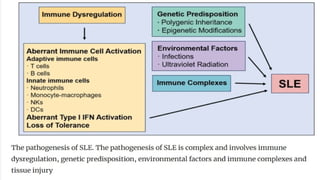
Pathogenesis of
SLE
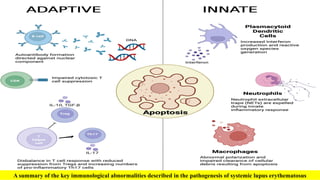
Immune dysregulation
Includesdysregulation or disruption of both innate and
adaptive immune systems. This disruption is involved in
the development and progression of disease.
The innate immune system’s dysfunction, which includes
reduced neutrophil phagocytic capacity and increased
oxidative stress, is accompanied by a buildup of dendritic
cells (DCs) at inflammatory locations, and defects or
mutations in the complement system, are linked to SLE.
Additionally, the abnormal function of adaptive
immunity, such as augmented B cell activity, failure in
the clearance of autoreactive B cells, and the
overactivation of T cells, can lead to an upsurge in
autoantibody production.
Studies have indicated that elevated levels of type I
interferons (IFNs) like alpha and beta are detectable in
SLE and are associated with the severity of the disease.
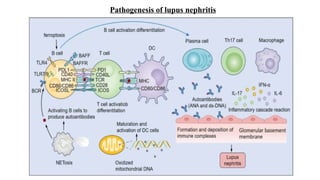
In SLE, thepathogenesis of lupus nephritis involves an intricate interplay among B cells, T
cells, DCs, and other immune components.
include:
(1) Excessive production of autoantibodies by aberrant B cells leads to the formation of
immune complexes, which deposit in the kidneys, activating the complement system and
inciting inflammatory responses.
(2) Autoreactive B cells present self-antigens to T cells, perpetuating immune dysregulation
and fostering the release of pro-inflammatory mediators.
(3) Dendritic cells exhibit aberrant recognition and presentation of self-antigens (dsDNA-
Sm antigen-Histones in drug-induced lupus) thereby initiating and propagating autoimmune
responses against renal tissue.
Understanding these pathogenic mechanisms is pivotal for the development of novel
therapeutic strategies aimed at halting or reversing the progression of lupus nephritis
31.
1
-
Aberrant immune cellactivation
• T cells may suffer a loss of self-tolerance, resulting in the stimulation of B
cells by autoreactive cells.
• This activation leads to an overproduction of autoantibodies by B cells,
which then form immune complexes.
• These complexes accumulate in tissues, initiating an inflammatory
response.
• Innate immune cells, such as neutrophils, monocyte-macrophages, natural
killer cells and DCs, also contribute significantly to SLE pathogenesis
• This interplay between adaptive and innate immune cells, along with the
overproduction of pro-inflammatory cytokines and the disruption of
regulatory mechanisms, culminates in chronic inflammation and multi-organ
damage characteristic of SLE.
32.
B-cell
• The rangeof autoantibodies generated by B cells with autoreactive
properties is primarily targeted against Self - antigens found in the cell
nucleus.
• In SLE, the abnormal stimulation of TLR9 and TLR7 has been shown to
markedly increase the generation of autoantibodies that target double-
stranded DNA (dsDNA) autoantigens.
• B lymphocytes have been demonstrated to act as antigen-presenting cells
(APCs) to T lymphocytes with autoreactive potential so produce
proinflammatory cytokines.
Role of the Complement System
• Complement dysfunction is proposed to accelerate several steps in the
pathogenic pathways of SLE, such as impaired clearance of apoptotic debris,
increased autoreactive CD+8 T cell activity (CTL) , and tissue damage by
activation of the inflammatory cascade in organs with IC deposition.
33.
T-cell
• Autoreactive Tcells are pivotal in the development of SLE.
• T-helper 1 (Th1) cells are involved in SLE pathogenesis, as they foster oxidative
stress linked to the production of interferon-gamma (IFN-γ) (activate
macrophage to produce proinflammatory cytokines)
• T-helper 17 (Th17) cells play a role in the pathogenesis of SLE, acting as the
main producers of IL-17, a highly inflammatory cytokine.
• This cytokine promotes the recruitment of neutrophils, triggers the activation
of the innate immune system, and enhances the functionality of B
lymphocytes.
• T-follicular helper (Tfh) cells are associated with the expansion of autoreactive
B-cell clones.
• CD8 T lymphocytes in the peripheral blood of SLE patients exhibit functional
deficits, such as an impaired ability to lyse target cells and a reduction in the
synthesis of granzymes and perforins.
• There is interaction between CD4 T cells and B cells in the development of
autoimmune conditions.
34.
Neutrophils
Neutrophils exhibit adiminished capacity for phagocytosis and a failure to clear apoptotic
cells, which are a source of self-antigens typically sequestered from the immune system.
Neutrophils have been shown to produce type-I IFNs which can lead to abnormal B-cell
development within the bone marrow of SLE patients.
A particular subtype of neutrophils, referred to as low-density granulocytes (LDG), is
commonly found in higher numbers in the peripheral circulation of SLE patients.
(LDGs) are distinguished by their heightened capacity to produce neutrophil extracellular
traps (NETs), particularly during the process of NETosis.
Neutrophils are known for generating reactive oxygen species (ROS), which, while typically
crucial for pathogen elimination, can inflict endothelial damage in SLE.
Excessive NET formation coupled with impaired clearance may also result in activation of
macrophages, thereby exacerbating the inflammatory response
In aggregate, these findings contributes to immune dysregulation and subsequent tissue
injury.
DCs
Bridge the innate and adaptive immune responses because it act as APC.
35.
A summary ofthe key immunological abnormalities described in the pathogenesis of systemic lupus erythematosus
36.
2-Aberrant type IIFN activation
In SLE, it is primarily the type-I IFN, particularly IFNα and IFNβ, that is
implicated in disease pathogenesis.
Studies using animal models demonstrated that administration of type-
I IFNs could induce autoantibody production and lead to organ
damage.
Type one interferon might play a pivotal part in SLE development in
humans came from observations that patients treated with IFNα for
hepatitis C or malignancies could develop antinuclear antibodies.
3-Loss of tolerance
The collapse of immune tolerance plays a pivotal role in the
development of autoimmune conditions such as SLE due to different
triggers as mentioned before.
Diagnosis of SLE
Thediagnosis of SLE is based on:
Characteristic clinical findings of the skin, joints, kidneys, and
the central nervous system. (primary diagnostic tool)
Serological parameters (Immunological Tests) such as
antinuclear antibodies (ANA), Anti–double-stranded DNA (anti-
dsDNA), Anti-Smith (anti-Sm), Anti-histone antibodies, Anti-
phospholipid antibodies and Complement Levels (C3 & C4).
Other Investigations (Imaging and Biopsies) like Urinalysis,
CBC, ESR/CRP and Biopsy (renal/skin).
40.
Serological parameters (ImmunologicalTests or Laboratory diagnostics )
Antinuclear antibody (ANA):
•Highly sensitive (~95–99%) but not specific, can occur in other autoimmune disease
like RA (A good screening test but not confirmatory)
Anti–double-stranded DNA (anti-dsDNA):
•High specificity, correlates with disease activity and nephritis.
Anti-Smith (anti-Sm):
•Highly specific but less sensitive.
Anti-histone antibodies:
•Associated with drug-induced lupus.
•Anti-phospholipid antibodies:
•e.g., lupus anticoagulant, anticardiolipin,anti-β2 glycoprotein I → linked to thrombosis
and pregnancy loss.
•Complement levels (C3, C4):
•Often low during active disease.
41.
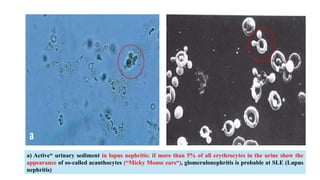
a) Active“ urinarysediment in lupus nephritis: if more than 5% of all erythrocytes in the urine show the
appearance of so-called acanthocytes (“Micky Mouse ears“), glomerulonephritis is probable at SLE (Lupus
nephritis)
42.
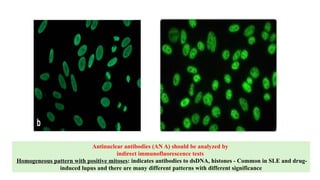
Antinuclear antibodies (ANA) should be analyzed by
indirect immunofluorescence tests
Homogeneous pattern with positive mitoses: indicates antibodies to dsDNA, histones - Common in SLE and drug-
induced lupus and there are many different patterns with different significance
43.
Other Investigations
• Urinalysis:proteinuria, casts → detect nephritis.
• CBC (Hematologic): anemia, leukopenia, thrombocytopenia.
• ESR/CRP: ESR often elevated; CRP usually normal unless infection.
• Biopsy (renal/skin): may be done to confirm lupus nephritis or cutaneous
lupus.
Like In the case of cutaneous manifestations, a dermatologist should be
consulted for a biopsy of the skin and/or oral mucous membrane lesions
(histology/ immunofluorescence) for purposes of differential diagnosis.
• Imaging by MRI and Ultrasound like in case of Lupus nephritis
Ultrasound assesses kidney size and MRI: may detect vascular changes.
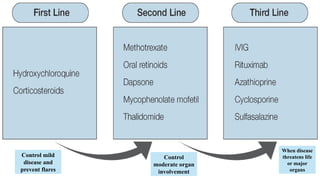
Pharmacological Management
Antimalarials=Cornerstone ofSLE therapy
• Antimalarials are among the oldest drugs used to treat SLE.
• Effective in the management of skin manifestations and arthritis.
• Hydroxychloroquine (HCQ) which decreasing lupus flares.
Glucocorticosteroids (GCs)
• Contributed to an increase in the survival rates of patients with SLE by broad suppression of inflammation
& immune system.
• The increasing concerns about the toxicity and severe side effects of GC have fostered the development of
alternative therapeutic strategies.
Conventional Immunosuppressive Agents
• Along with their immunomodulatory properties, they also allow a more rapid and successful decreacing of
GC dose.
• The combined therapy with GCs and cyclophosphamide (CYC), compared to GC monotherapy, led to a
better renal outcome and to a higher remission rate in patients.
47.
NSAIDs
• Symptomatic relief(inflammation, pain, fever) → mild, localized disease.
Targeted Therapies: Biologic Agents
• RTX is a chimeric monoclonal Ab which selectively targets B cell-specific surface
molecule (CD20) and thus reduces autoantibody production and abnormal immune
activation.
• Belimumab, a fully humanized monoclonal antibody which inhibits B lymphocyte
stimulator (BAFF).
Adjuvant Treatments
• Intravenous immunoglobulins (IVIGs), which are purified from the plasma of healthy
human donors.
• The association of IVIG administration with significant improvement in disease activity
scores and complement levels
• Therapeutic plasma exchange (TPE) is a blood purification technique used for the
removal of pathological substances, such as auto-Ab and replacement with a pure
blood.