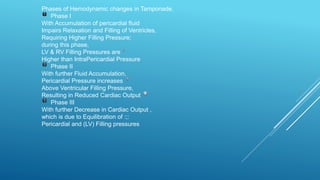
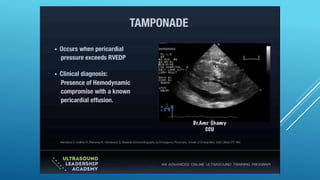
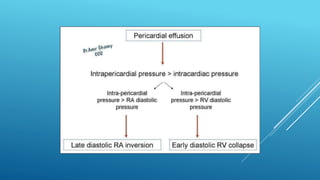
The document describes three phases of hemodynamic changes that occur in cardiac tamponade:
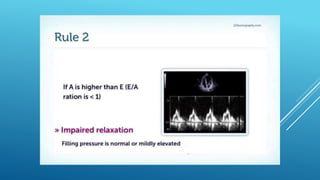
Phase I involves accumulation of pericardial fluid that impairs ventricular filling and relaxation, requiring higher filling pressures. Left and right ventricular filling pressures are higher than intrapericardial pressure.
Phase II further fluid accumulation causes pericardial pressure to increase above ventricular filling pressures, resulting in reduced cardiac output.
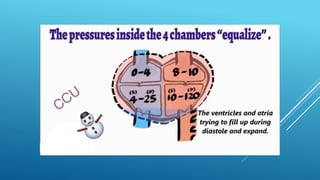
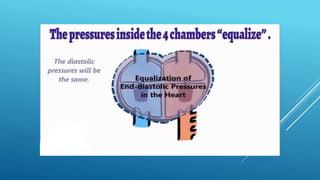
Phase III shows further decrease in cardiac output due to equalization of pericardial pressure and left ventricular filling pressure.















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
