2. Objectives
● Introduction.
● Types of TAPVR.
● Symptoms of TAPVR.
● Causes and Risk Factors.
● Pathophysiology
● Diagnosis
● Medical Management
● Surgery
● Complication of TAPVR
3. INTRODUCTION
Pulmonary veins are four in number and carry oxygenated blood from lungs to the left atrium of the heart .
The anatomy of the pulmonary veins is variable with some anatomic variants.
The difference between the normal anatomy of pulmonary veins with its variants and anomalous anatomy is
important in clinical practice and sometimes can be challenging for clinicians. Variants of pulmonary veins may
occur in number, diameter, and normal venous return.
The pulmonary venous return can deviate from the usual anatomical configuration and ranges from normal
variant drainage to anomalous pulmonary-systemic communications .
This means that the pulmonary veins are directly connected to the systemic venous circulation by maintaining a
connection to the splanchnic circulation. The anomalous pulmonary venous return is divided into partial and total
anomalous pulmonary venous return (TAPVR).
Total anomalous pulmonary venous return (TAPVR) is a rare and critical congenital vascular anomaly, makes up
1.5% (1–3%) of congenital cardiac disease and the prevalence rate reaches up to 0.8/10.000 of live births
4. Types of TAPVR
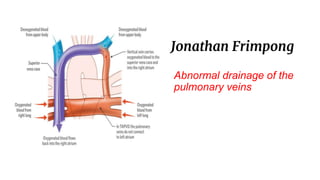
• Supracardiac– In supracardiac TAPVR, the pulmonary veins come together and form
an abnormal connection above the heart to the superior vena cava, which is a main
blood vessel that brings oxygen-poor blood from the upper part of the body to the heart.
In this type of TAPVR, a mixture of oxygen-poor and oxygen-rich blood returns to the
right atrium through the superior vena cava.
• Cardiac – In cardiac TAPVR, the pulmonary veins meet behind the heart and connect to
the right atrium. The coronary sinus, which is a vein that helps bring oxygen-poor blood
from the heart muscle back to the heart, helps connect the pulmonary veins to the right
atrium in this type of TAPVR.
• Infracardiac – In infracardiac TAPVR, the pulmonary veins come together and form
abnormal connections below the heart. A mixture of oxygen-poor blood and oxygen-rich
blood returns to the right atrium from the veins of the liver and the inferior vena cava,
which is the main blood vessel that brings oxygen-poor blood from the lower part of the
body to the heart
5. Symptoms of TAPVR
• Newborns with TAPVR will have blue coloring of their skin, lips, and
cyanosis. This happens in the first hours or days of their life.
Other symptoms can be a bit different for each child. They can include:
• Fast or troubled breathing
• Fast heart rate
• Cool, clammy skin
• Tiredness and little movement
• Poor feeding
• Poor pulses
• Enlarged liver
• Heart murmur
6. Causes and Risk Factors
• The causes of heart defects, such as TAPVR, among most babies are
unknown.
• Some babies have heart defects because of changes in
their genes or chromosomes.
• Heart defects also are thought to be caused by a combination of genes
and other risk factors, such as the things the mother or fetus come in
contact with in the environment
• Medicines
7. Pathophysiology
Total anomalous pulmonary venous
return (TAPVR) is a birth defect of
the heart. In a baby with TAPVR,
oxygen-rich blood does not return from
the lungs to the left atrium. Instead,
the oxygen-rich blood returns to the
right side of the heart. Here, oxygen-
rich blood mixes with oxygen-poor
blood.
8. Diagnosis
Chest X-ray
A chest X-ray may show changes in the heart and lungs caused by TAPVR.
Electrocardiogram (ECG)
An ECG records the electrical activity of the heart. It also shows abnormal rhythms (arrhythmias) and finds
heart muscle stress. These problems may be caused by TAPVR.
Echocardiogram (echo)
An echo can show the structural changes of TAPVR and abnormal connections of the pulmonary veins.
Cardiac catheterization
A cardiac catheterization gives detailed information about the structures in the heart.
CT and magnetic resonance angiography (MRA)
A CT and MRA can show detailed information about the pathways and connections of the pulmonary veins.
Angiographic computerized tomography (angioCT)
9. Medical Management
• Supplemental oxygen or ventilator
• Prostaglandin therapy- Prostaglandin E1
• ECMO (extracorporeal membrane
oxygenation). This method gives both
cardiac and respiratory support for
babies
• Cardiac catheterization- balloon atrial
septostomy
10. Surgery
• The goal of the surgical repair of TAPVR is to restore normal blood flow
through the heart. To repair this defect, surgeon usually connect the
pulmonary veins to the left atrium, close off any abnormal connections
between blood vessels, and close the atrial septal defect.
• The surgery is done through a cut (incision) through the breastbone
(sternum)
11. Complications of TAPVR
•Enlarged heart
•Lung problems, including respiratory failure and high blood pressure in
the lungs
•Abnormal heart rhythms
•Shock
•Heart failure
•Slowed growth and development
•Enlarged liver
•Need for another surgery
•Infection
•Death