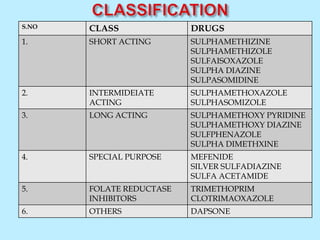
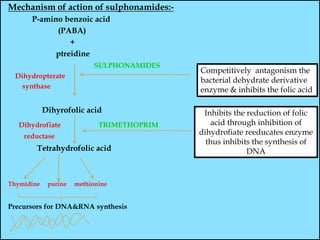
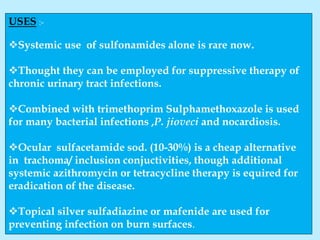
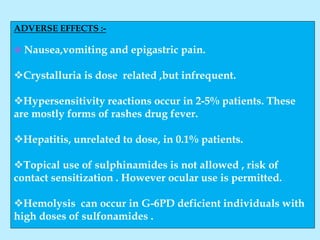
This document summarizes information about sulphonamides, including their classification, mechanism of action, pharmacokinetics, uses, and adverse effects. Sulphonamides were the first effective chemotherapeutic agents used to treat bacterial infections. They work by competitively inhibiting the bacterial enzyme dihydropteroate synthase, blocking the synthesis of folic acid and DNA. Different sulphonamides have short, intermediate, or long durations of action depending on their absorption and excretion rates. While systemic use is now rare, sulphonamides combined with trimethoprim or used topically to prevent infections remain important. Adverse effects can include nausea, crystalluria, and hypersensitivity reactions.