EXTERNAL HORDEOLUM (STYE)
Defn: An acute suppurative inflammation of gland of the Zeis or Moll.
Causative organism -Staphylococcus Aureus
Predisposing factors
Habitual rubbing of the eyes
Fingering of the lids and nose,
Chronic blepharitis and
Diabetes mellitus
Excessive intake of carbohydrates and alcohol.
3.
Individuals with
diabetes aregenerally
prone to acute
infections of any
kind especially when
there is uncontrolled
diabetes.
The eyelids are
more susceptible to
infection and, hence,
ulcerative blepharitis
and styes are more
commonly found in
diabetes patients.
Why are
people with
diabetes more
prone to
infections?
High blood sugar levels can
weaken a person's immune
system defenses. People
who have had diabetes for a
long time may have
peripheral nerve damage
and reduced blood flow to
their extremities, which
increases the chance for
infection.
4.
Symptoms
Acutepain
swelling of lid
Mild watering
Photophobia.
Signs
Stage of cellulitis -localised, Hard, red, tender swelling at the lid
margin associated with marked oedema
Stage of Abscess formation -visible pus point on the lid margin in
relation to the affected cilia.
Usually there is one stye, but occasionally, these may be multiple.
5.
Treatment
Hot compresses2-3 times a day are very useful in
cellulitis stage.
When the pus point is formed it may be evacuated by
Epilating the involved cilia.
Surgical incision is required rarely for a large abscess.
Antibiotic eyedrops (3-4 times a day) and
Eye ointment (at bed time).
Anti-inflammatory and analgesics relieve pain and
reduce oedema.
Systemic antibiotics may be used for early control of
infection.
6.
CHALAZION
Tarsal OrMeibomian Cyst.
Defn: It is a Chronic non-infective granulomatous inflammation
of the Meibomian gland.
Pathology
Low grade of
infection
Accumulation
of meibomian
secretion
Obstruction
of ducts
7.
Clinical picture
Painlessswelling in the lid
A feeling of mild heaviness.
Nodule-small, firm to hard, non-tender swelling present
slightly away from the lid margin.
Drooping of eyelid in multiple/large Chalazion.
Upper lid is more involved than the lower.
On everting the lid-a reddish purple area is seen on palpebral
conjunctiva after of eversion of lids.
8.
Complications
Slowly increasesin size and
becomes very large.
A large chalazion of the upper lid
may press on the cornea and cause
blurred vision.
A large chalazion of the lower lid
may rarely cause eversion of the
punctum or even ectropion and
epiphora
Ptosis
Incision and curettage
Topical anaesthesia-
Instillation of xylocaine drops in the eye
Chalazion is infiltrated with 2 percent xylocaine solution.
Incision is made with a sharp blade, which should be vertical on
the conjunctival side .
The contents are curetted out with the help of a chalazion scoop.
To avoid recurrence, its cavity should be cauterised with carbolic
acid.
An antibiotic ointment is instilled and eye padded for about 12
hours.
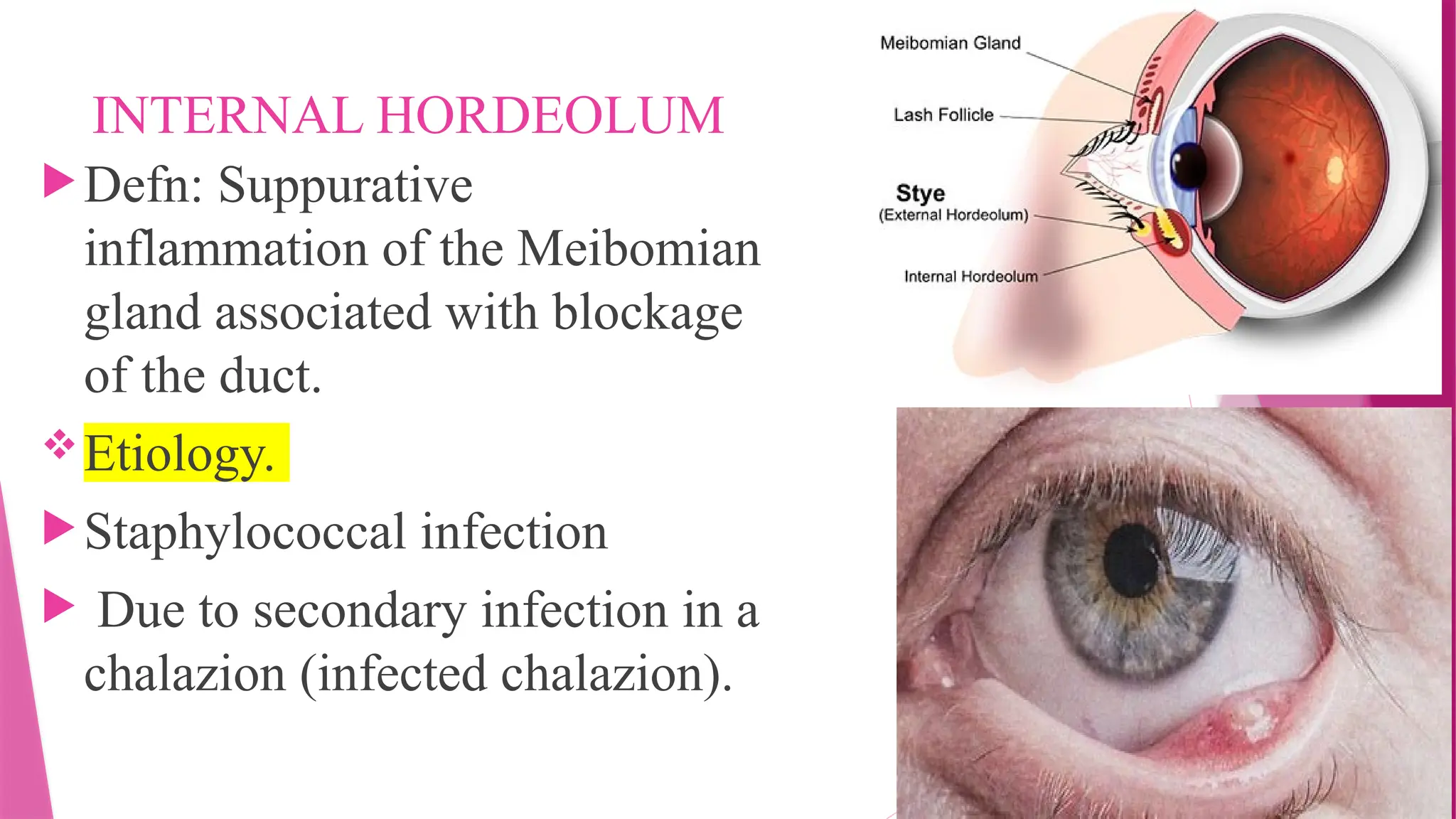
INTERNAL HORDEOLUM
Defn: Suppurative
inflammationof the Meibomian
gland associated with blockage
of the duct.
Etiology.
Staphylococcal infection
Due to secondary infection in a
chalazion (infected chalazion).
14.
Clinical picture
Similarto hordeolum externum, except that pain
is more intense,
Mild watering
Photophobia
Localizes Firm, Red,tender, Swelling of Lid with
marked oedema
15.
Treatment.
It issimilar to Hordeolum Externum
except that, when the pus is formed, it should be drained
by a vertical incision from the tarsal conjunctiva
THANK
YOU….