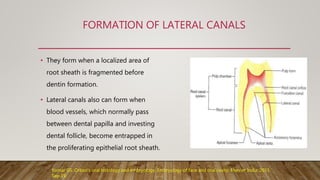
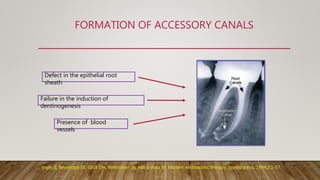
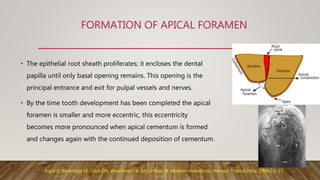
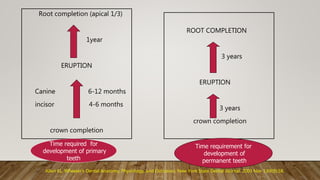
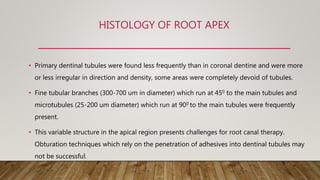
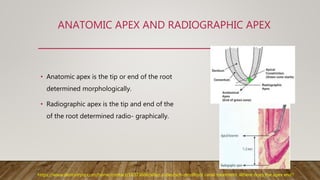
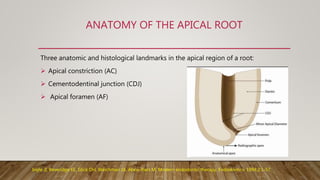
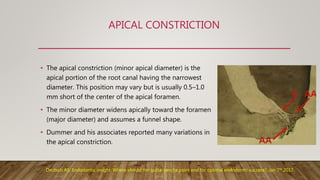
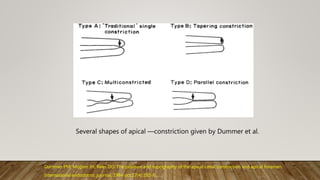
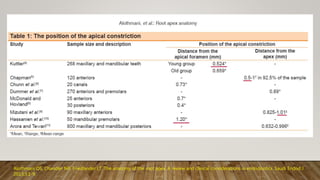
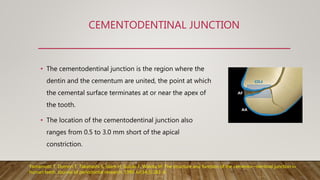
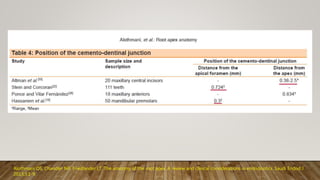
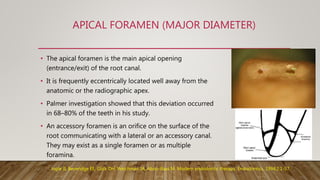
The document discusses the anatomy and histology of the root apex. It describes the development of root structures including the apical constriction, cementodentinal junction, and apical foramen. Variations in root apex morphology are discussed including accessory canals, resorption, and calcifications. The clinical significance of understanding root apex anatomy for procedures like working length determination, apical resection, and apexification are summarized.