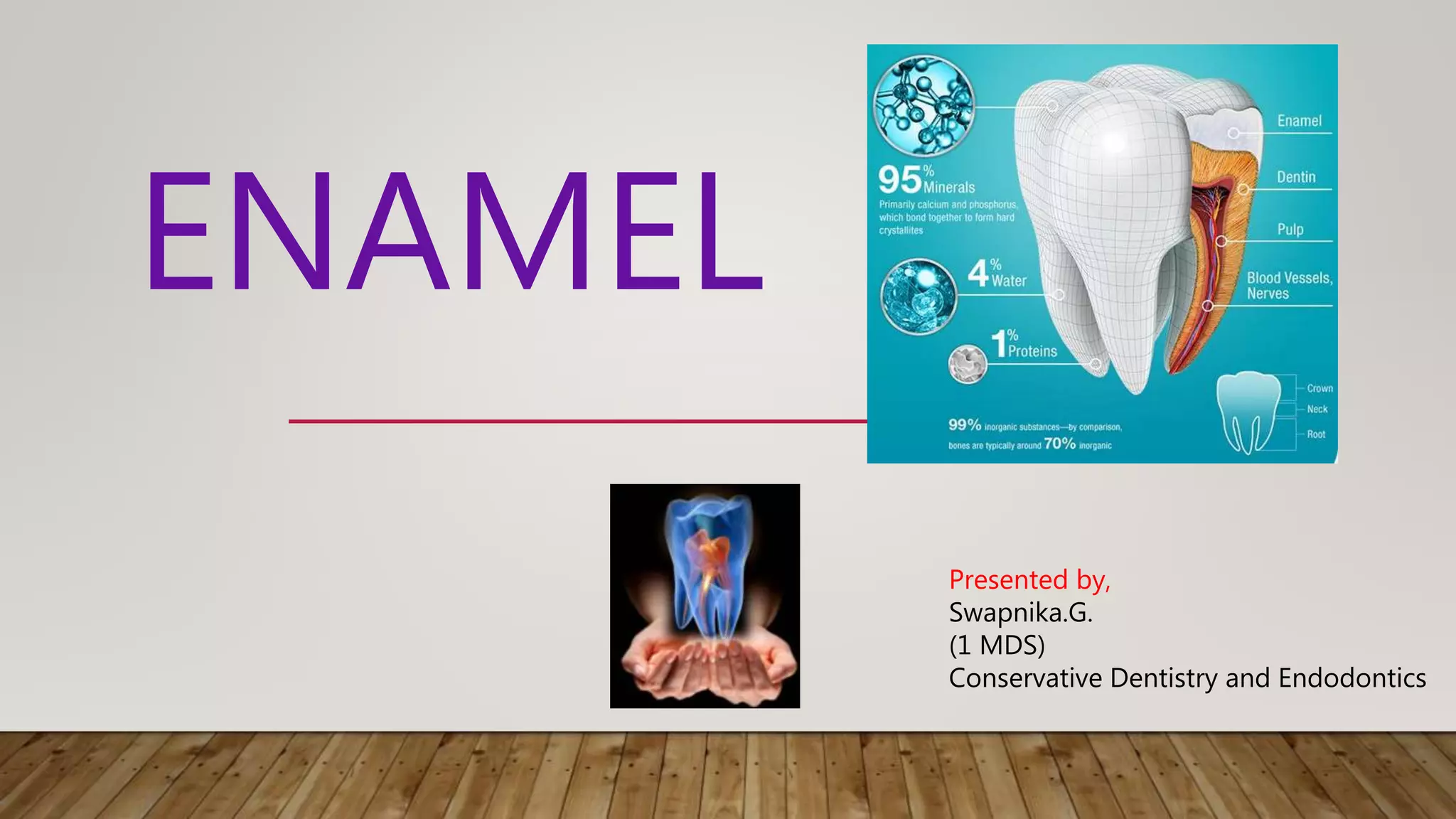
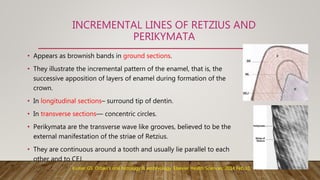
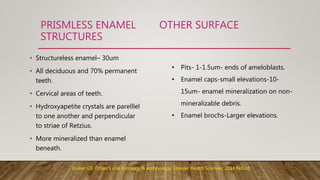
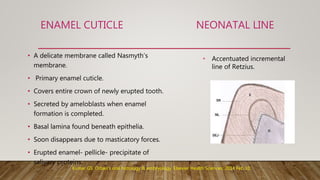
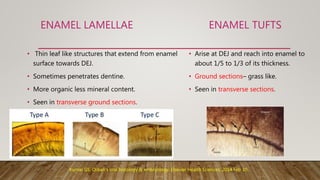
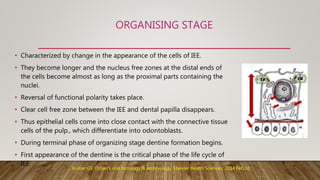
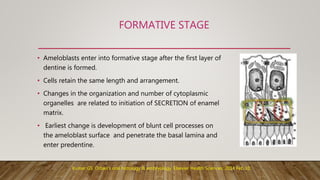
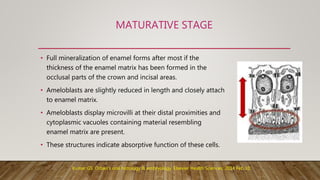
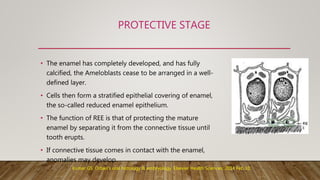
This document provides an overview of the structure and properties of enamel. It discusses the physical and chemical composition of enamel, including its high mineral content and hydroxyapatite crystals. It describes the microscopic structure of enamel, including enamel rods, interrod enamel, and surface features like striations of Retzius. It also summarizes the life cycle of ameloblasts and the process of amelogenesis. Bleaching effects on enamel and developmental disturbances are briefly covered.