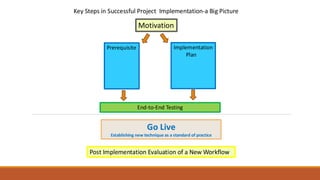
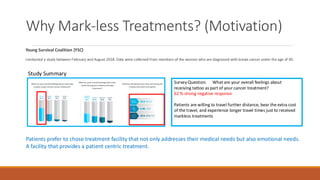
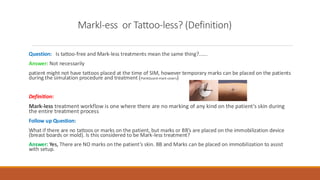
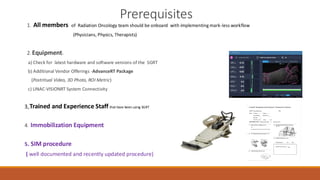
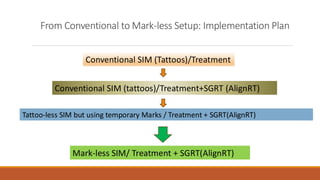
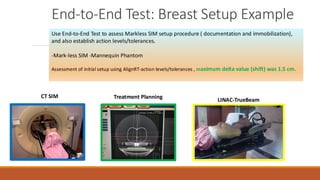
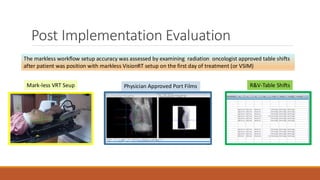
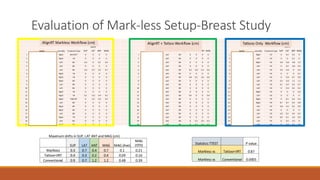
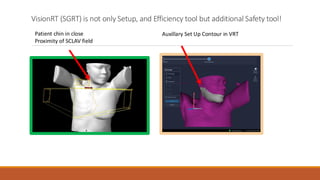
The presentation describes how a community hospital with limited resources successfully implemented a fully mark-less setup workflow for all treatment sites using SGRT. It emphasizes patients' preference for tattoo-free treatments, outlines a step-by-step implementation plan, and presents data showing that the mark-less setup achieves accuracy comparable to workflows using tattoos plus SGRT—reinforcing SGRT’s value not only for setup and efficiency, but also as a safety-enhancing tool.