Downloaded 15 times
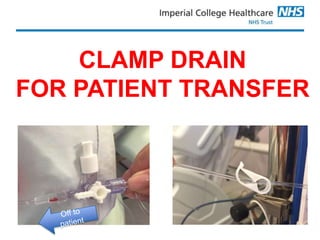
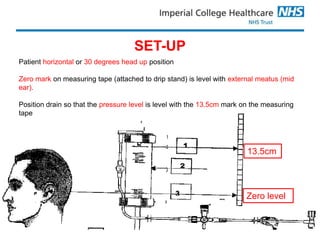




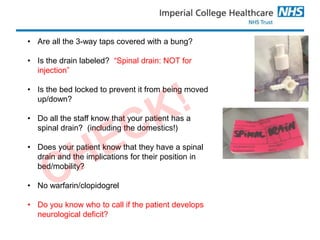

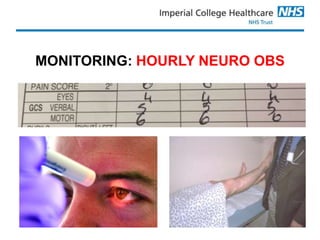



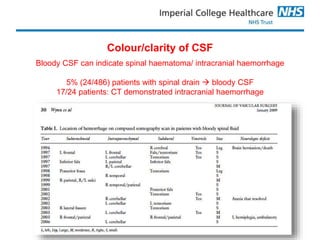



This document provides guidelines for managing spinal drains post-operatively. It states that the drain should be set up so that the drainage chamber is 13.5cm above the spinal cord to allow drainage of CSF if pressure rises above normal. It emphasizes that the drain and patient must not be moved without clamping the drain to avoid complications. It outlines important monitoring parameters, signs that indicate issues like increased CSF drainage, and procedures for drain removal and resuming anticoagulation.


























































