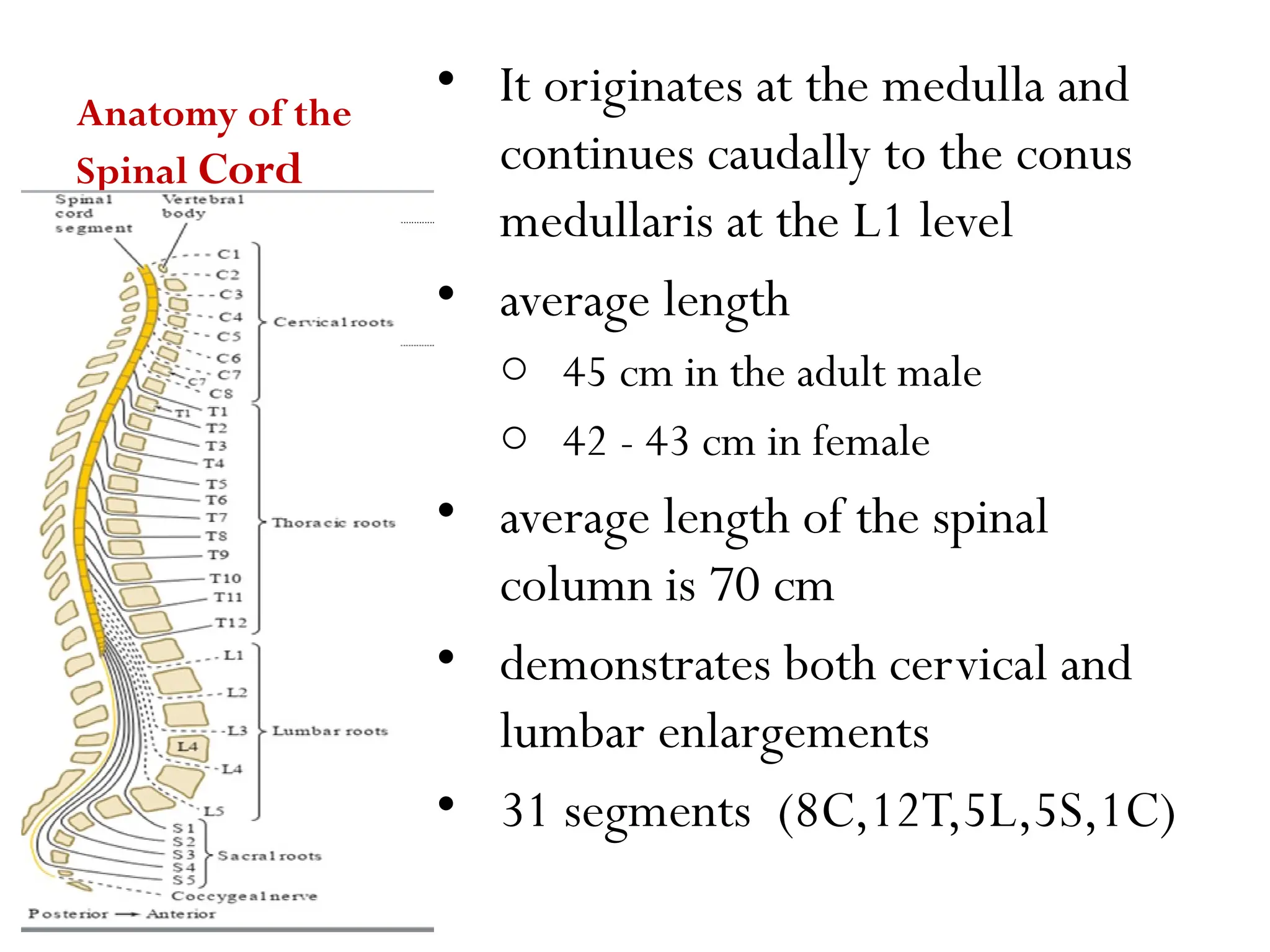
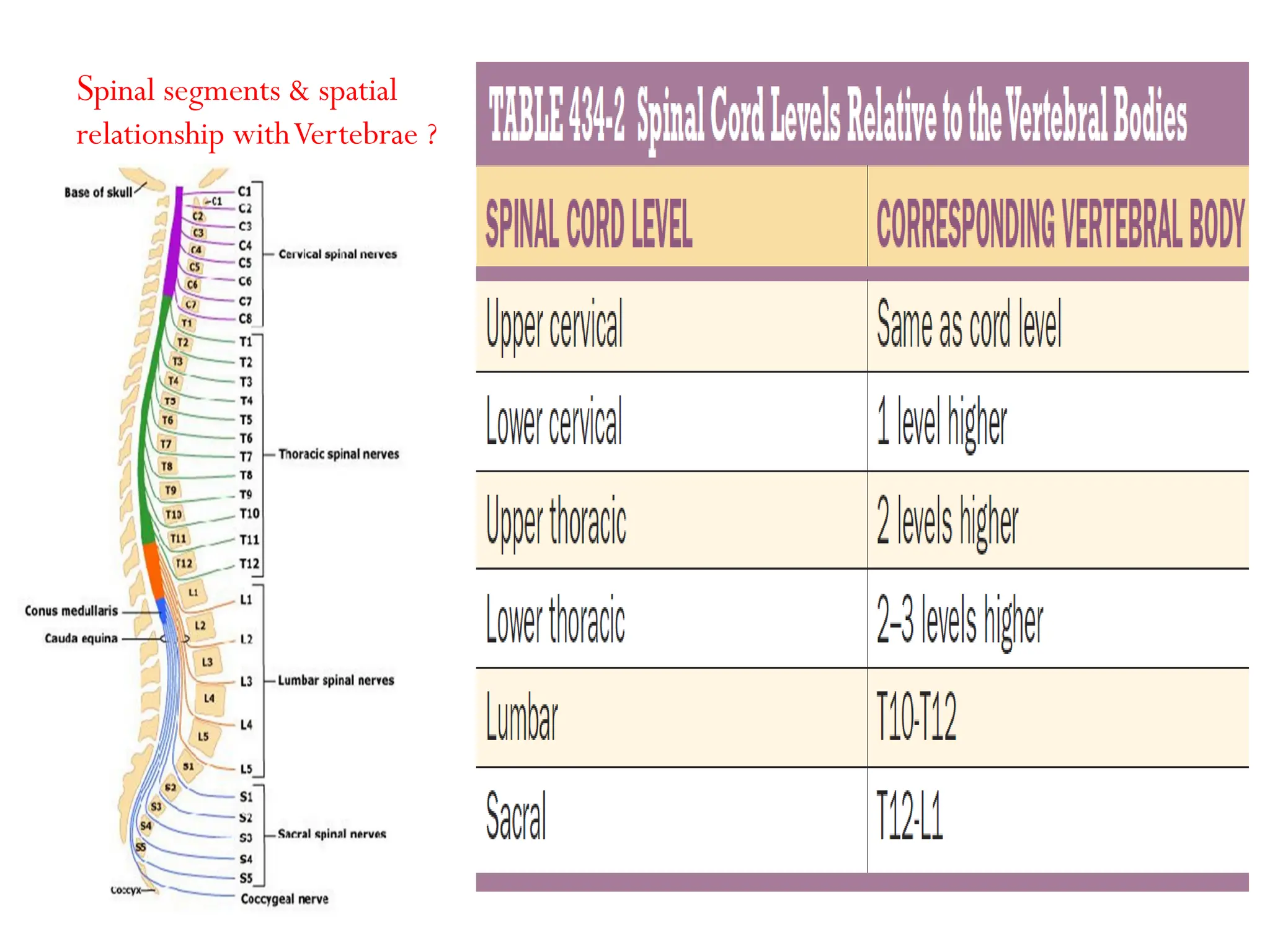
The document provides a detailed overview of spinal cord disorders, their anatomy, and associated pathologies, including descriptions of various syndromes such as complete spinal cord transection, Brown-Séquard syndrome, central cord syndrome, and anterior spinal artery syndrome. It outlines clinical cases highlighting symptoms and diagnoses, explaining the implications of spinal cord lesions, their classifications, and neurological implications. Additionally, it discusses the arterial supply, venous drainage, and pain mechanisms associated with spinal cord disorders.