Downloaded 12 times



























![Cardio-Vascular Clinical Results
time [s]
CT [HU]
time [s]
CT [HU]
3B
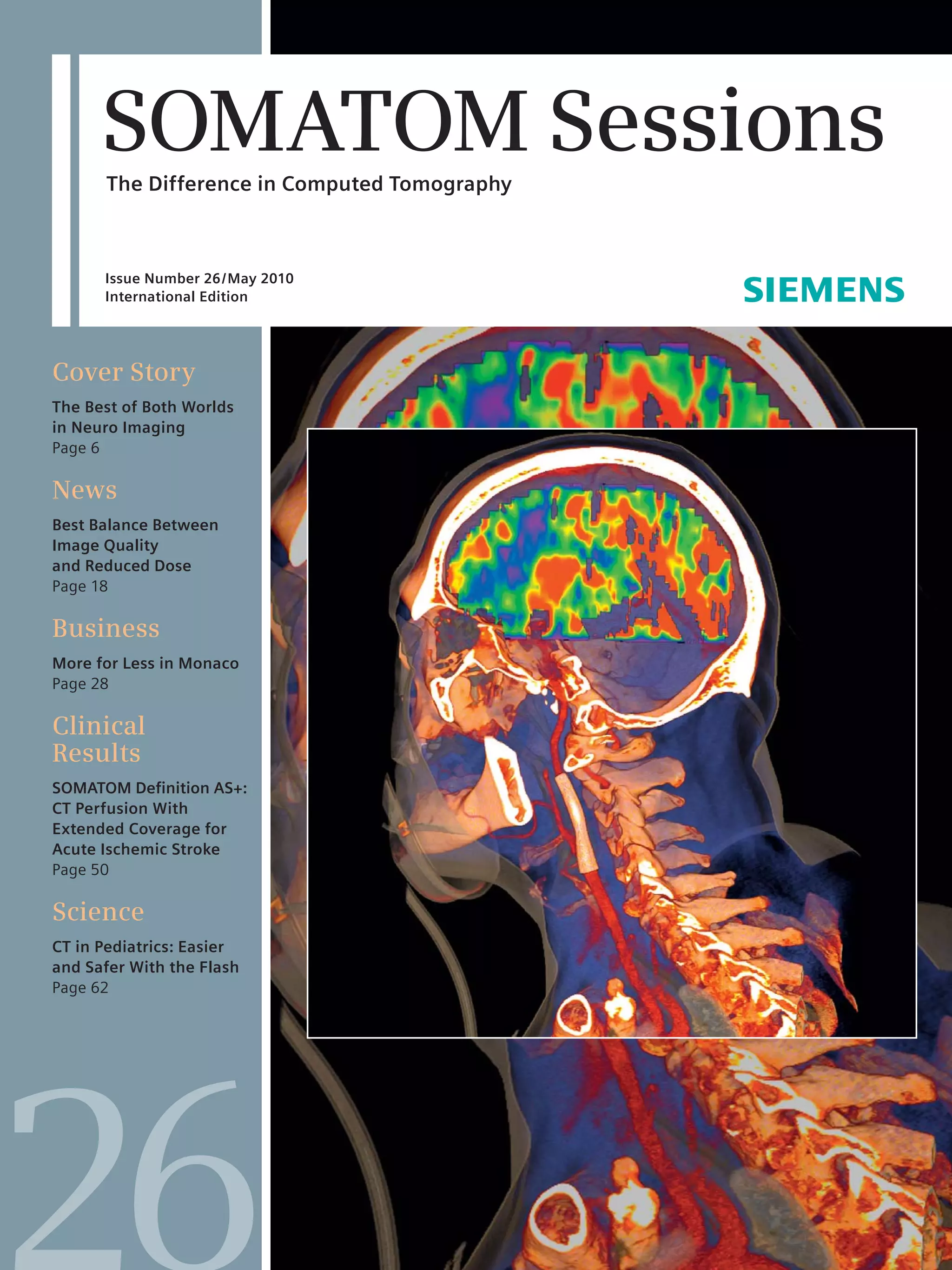
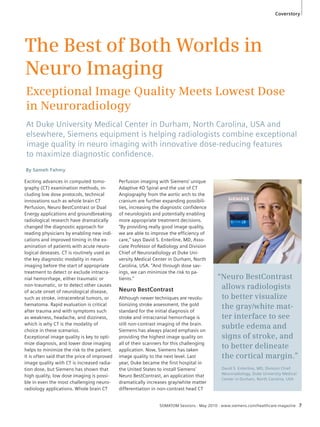
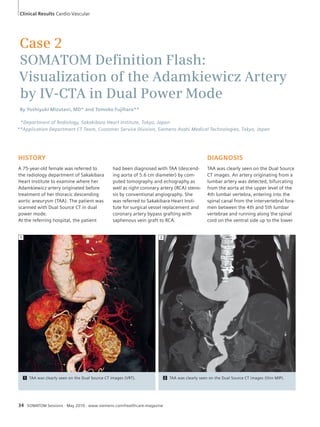
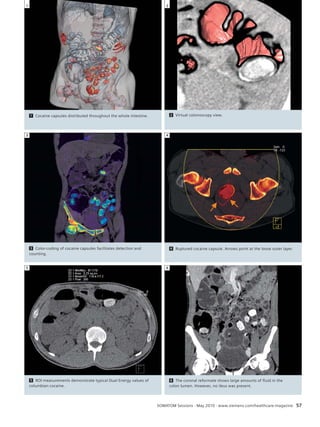
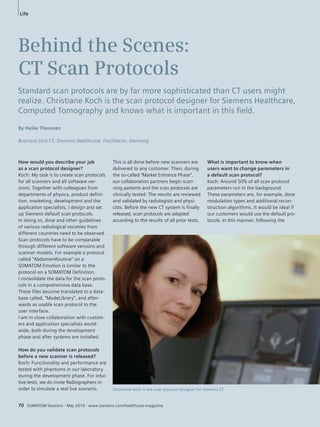
3 Principle: dynamic volumetric myocardial stress perfusion to quantify Myocardial Blood Flow (MBF). Comparison of different time
attenuation curve (TCA) pattern with a slower and lower peak (86 ml / 100 ml / min) in an ischemic segment (Fig. 3A) and normal blood flow
(MBF 159 ml / 100 ml / min) in an healthy segment (Fig. 3B).
SOMATOM Sessions · May 2010 · www.siemens.com/healthcare-magazine 37
EXAMINATION PROTOCOL
Scanner SOMATOM Definition
Scan mode Dynamic Stress Perfusion Mode Dose modulation no
Scan area Left ventricular myocardium CTDIvol 94.15 mGy
Scan length 72 mm Rotation time 0.28 s
Scan direction Cranio-caudal Slice collimation 32 x 1.2 mm
Scan time 31 s Slice width 3 mm
Heart rate 72 bpm Reconstruction increment 2 mm
Tube voltage 100 kV Reconstruction kernel B23f
Tube current 350 mAs/rot. Post processing syngo VPCT
Body Myocardium
4 Systolic reconstruction display of long axis, color-coded myo-cardial
stress perfusion image of the left ventricle indicating homo-geneous
perfusion (green) and the absence of a circumscribed
perfusion defect.
4
5 Short axis color-coded perfusion map of the left ventricle
demonstrating homogeneous perfusion (green) under
adenosine stress.
5
3A
80
60
40
20
0
0 5 10 15 20 25 30
100
80
60
40
20
0
0 5 10 15 20 25 30](https://image.slidesharecdn.com/somatomsessions26int-00079316-00270153-140821164210-phpapp01/85/Somatom-sessions-26-37-320.jpg)
![Clinical Results Cardio-Vascular
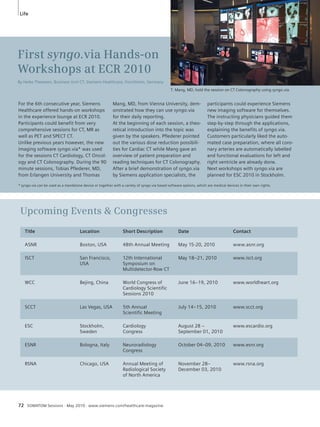
Case 4
Pre-operative Exclusion of Coronary
Artery Stenosis With Less Than 1 mSv Dose
By Sebastian Leschka, MD* and Andreas Blaha**
Institute of Diagnostic Radiology, University Hospital Zurich, Zurich, Switzerland
Business Unit CT, Siemens Healthcare, Forchheim, Germany
HISTORY
A 71-year-old male patient with a history
of cerebral infarction caused by a high-grade
stenosis of the left internal carotid
artery and lysis therapy was now re-ferred
to the radiology department to
rule out coronary artery disease.
In addition to the coronary CT Angio-graphy
(CTA) examination a non-en-hanced
calcium-scoring scan (CaSc)
was performed.
The CTA was acquired with a fast pitch
spiral technique (Flash Spiral Cardio)
while a mean heart rate of 56 bpm was
present.
38 SOMATOM Sessions · May 2010 · www.siemens.com/healthcare-magazine
COMMENTS
In combination with the CaSc (0.35 mSv)
and the CTA (0.8 mSv), an effective
dose* of 1.1 mSv was applied to the
patient to detect coronary artery disease.
The entire acquisition time of the CTA
was 280 ms; calcium scoring was
acquired in 120 ms.
The Flash Spiral cardio method quickly
and reliably combines low radiation
dose values with the accurate display of
the coronary arteries in all segments.
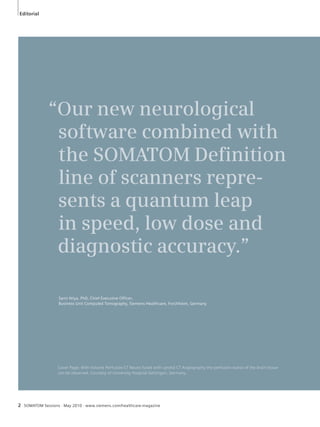
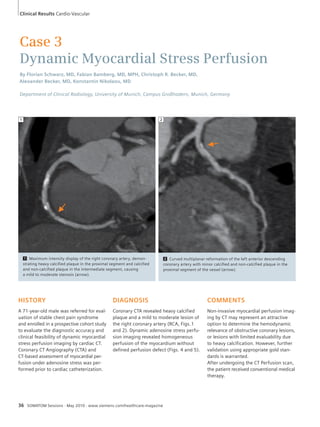
DIAGNOSIS
In total, ten calcified lesions could be
detected in the CaSc. Diffuse distribution
of calcified deposits was observed in
the right coronary artery (RCA), the left
artery descending (LAD) and the left cir-cumflex
coronary artery (CX). The total
Agatston score was 130.
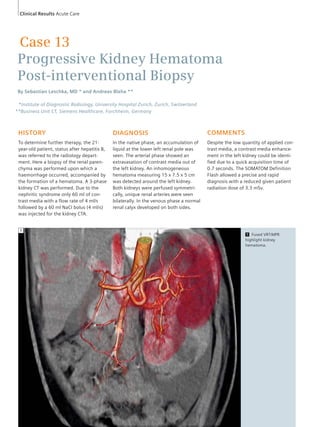
CTA unveiled a normal coronary artery
anatomy, right dominant coronary supply
type with regular sized lumen of the
coronary arteries. RCA and LAD showed
no hemodynamic relevant lesions. CX
coronary artery unveiled a stenosis
smaller than 50% in its proximal seg-ment.
A deep myocardial bridging of the
LAD could also be depicted.
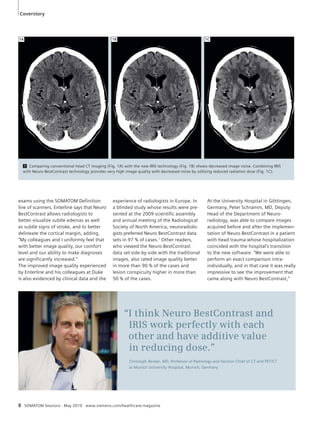
Threshold = 130 HU (102.7 mg/cm3 CaHA)
Artery Numbers of Calcium Score (2) Volume [mm3] (3) Equiv. Mass
Lesions (1) [mg CaHA] (4)
LM 0 0.0 0.00 0.0
LAD 2 27.5 29.3 4.89
CX 3 48.3 50.5 8.57
RCA 5 53.6 66.2 10.81
Total 10 129.5 146.0 24.27
(1) Lesion is volume based, (2) Equivalent Agatston score, (3) Isotropic interpolated volume, (4) Calibration Factor: 0.790
*Effective Dose was calculated using the published conversion factor for an adult chest of 0.014 mSv (mGy cm)-1 [1].
[1] McCollough CH et al. Strategies for Reducing Radiation Dose in CT, Radiol. Clin. N. Am. 47: (2009) 27-40.
*
**](https://image.slidesharecdn.com/somatomsessions26int-00079316-00270153-140821164210-phpapp01/85/Somatom-sessions-26-38-320.jpg)

![Clinical Results Cardio-Vascular
Case 5
Utilizing Ultra Low Dose
of 0.05 mSv for Premature Baby
With Congenital Heart Disease
By Jean-Francois Paul, MD1 and Andreas Blaha2
1Centre Chirurgical Marie Lannelongue, Le Plessis-Robinson, France
2Business Unit CT, Siemens Healthcare, Forchheim, Germany
HISTORY
A premature baby was referred to the
radiology department with diagnosis of
congenital heart disease. An atrial and
left ventricular septum defect could be
detected with echocardiography but
with a doubt about the exact origin and
*Effective Dose was calculated using the published conversion factor for a pediatric (newborn) chest of 0.039 mSv (mGy cm)-1 [1].
To take into account that Siemens calculates the CTDI in a 32 cm CTDI phantom an additional correction factor of 2 had to be applied.
[1] McCollough CH et al. Strategies for Reducing Radiation Dose in CT, Radiol. Clin. N. Am. 47: (2009) 27-40.
40 SOMATOM Sessions · May 2010 · www.siemens.com/healthcare-magazine
course of right pulmonary artery (RPA).
Therefore a low dose CT examination
was requested, utilizing low kilovoltage
(kV) and low milliampere seconds (mAs)
to achieve ultra low dose radiation
values.
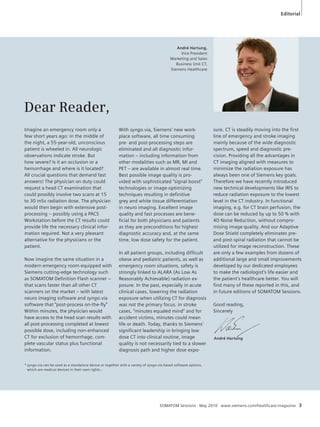
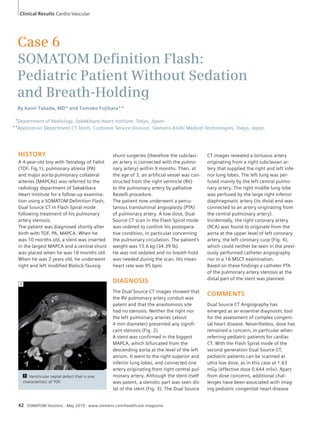
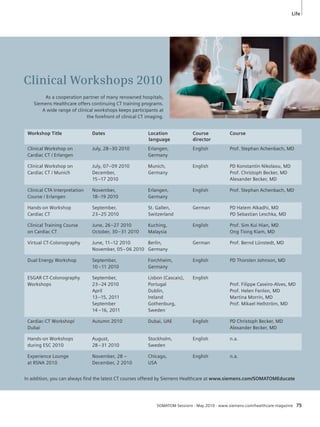
DIAGNOSIS
A mild stenosis present at the ostium
of the right pulmonary artery could be
observed. Although the RPA showed an
irregularity it had a normal anatomical
course. The ventricular septum defect as
well as the still open atrial septum could
be clearly revealed by using oblique pla-nar
reformations. The right coronary ar-tery
was well depicted despite a heart
rate of 157 bpm.
COMMENTS
The data acquisition was performed
with a SOMATOM Definition Flash using
the ECG-triggered sequential mode
(Flash Cardio Sequence) which resulted
in an ultra low dose value. Calculated
with the dose length product (DLP) of
0.7, an estimated dose of 0.05 mSv could
be achieved.*
Using the Definition Flash low dose ac-quisition
technique it was possible to de-tect
this congenital heart disease (CHD)
in a very early stage of the patients life.
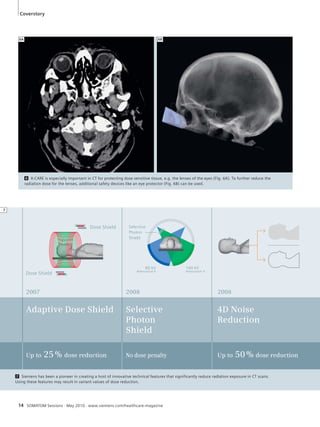
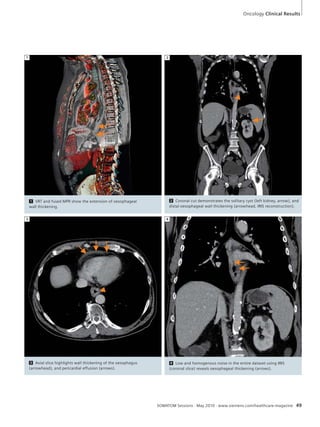
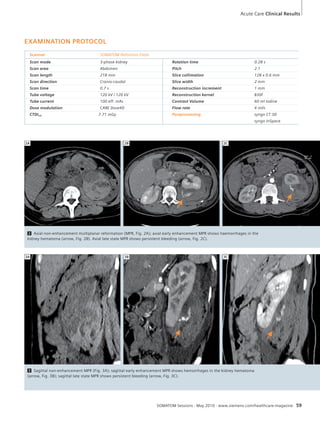
1 CT imaging with VRT technique shows ventricular septal defect (arrows)
and persistent foramen ovale (PFO, arrowheads).
1](https://image.slidesharecdn.com/somatomsessions26int-00079316-00270153-140821164210-phpapp01/85/Somatom-sessions-26-40-320.jpg)











![Acute Care Clinical Results
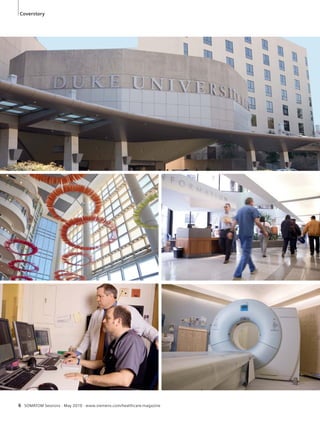
5 6 COMMENTS
EXAMINATION PROTOCOL
Scanner SOMATOM
Definition
Scan mode Thorax HiPitch
Scan area Thorax
Scan length 159 mm
Scan direction Cranio-caudal
Scan time < 1s
Tube voltage A/B 120 kV / 120 kV
Tube current A/B 10 eff. mAs
Dose modulation CARE Dose4D
CTDIvol 0.56 mGy
DLP 9 mGy cm
Effective Dose 0.37 mSv*
Rotation time 0.33 s
Pitch 3.0
Slice collimation 64 x 0.6 mm
Slice width 1.0 mm
Reconstruction
increment 0.5 mm
Reconstruction
kernel B60f
Postprocessing syngo CT 3D
syngo InSpace
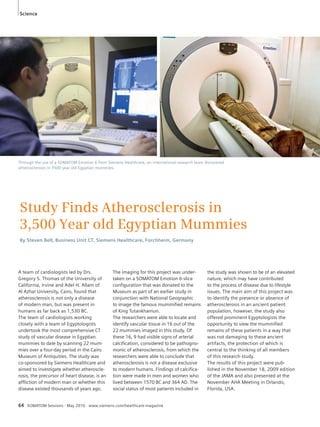
7 Volume rendered image of the thorax, showing regular bronchial tree.
SOMATOM Sessions · May 2010 · www.siemens.com/healthcare-magazine 61
7
6 Regular scan – sagittal image shows
motion artifact of the diaphragm due to
breathing during the acquisition.
5 High pitch scan – sharp delineation
of pulmonary segments.
Because of motion, the previous CT
scan made diagnosis more difficult
(Figs. 2, 4, 6). The fast acquisition
speed made it possible to reliably
rule out the presence of pulmonary
infiltrations and mycosis. Although
only 10 mAs were utilized, a high
diagnostic image quality was pre-served.
Using the new high pitch
scanning technique a significant re-duction
of radiation dose is feasible.
*Effective Dose was calculated using the published conversion factor for an 5-year-old pediatric chest of 0.082 mSv (mGy cm)-1 [1].
To take into account that Siemens calculates the CTDI in a 32 cm CTDI phantom an additional correction factor of 2 had to be applied.
[1] McCollough CH et al. Strategies for Reducing Radiation Dose in CT, Radiol. Clin. N. Am. 47: (2009) 27-40.](https://image.slidesharecdn.com/somatomsessions26int-00079316-00270153-140821164210-phpapp01/85/Somatom-sessions-26-61-320.jpg)





![Science
Scientifi c Validation of the
SOMATOM Defi nition Flash
One of the cornerstones of Siemens CT activities has always been the
scientifi c validation of Siemens’ products and solutions. Independent peer-review
of publications in scientifi c journals provides an unbiased and
objective assessment of the capabilities of the systems.
By Stefan Ulzheimer, PhD, and Peter Seitz
Business Unit CT, Siemens Healthcare, Forchheim, Germany
Since the introduction of the Siemens
SOMATOM Definition Flash at RSNA
2008, and its commercial availability in
July 2009, the CT scanner has been cov-ered
in 15 presentations at the annual
meeting of the Radiological Society
of North America in 2009 and ten peer-reviewed
publications in renowned
journals.
These presentations and publications
prominently feature the notable advan-tages
of the SOMATOM Definition Flash
that enhance efficiency and significantly
improve patient care.
Split-second Thorax – Lell et al. from
the University Hospital of Erlangen dem-onstrated
the SOMATOM Definition
Flash’s capabilities with its high-pitch
scan mode in thorax examinations.1
Twenty-four consecutive patients who
presented with chest pain received a
high-pitch thorax scan (Pitch 3.2) to
exclude coronary artery disease, pulmo-nary
embolism and aortic dissection.
The average dose was 1.6 mSv for pa-tients
who were scanned with a 100 kV
protocol and 3.2 mSv for patients who
were scanned with a 120 kV protocol.
The authors conclude that the “[…] high-pitch
scan mode allows motion artifact
free and accurate visualization of the
thoracic vessels and diagnostic image
quality of the coronary arteries in pa-tients
with low and stable heart rates at
a very low radiation exposure.”
The dose saving potential of the high-pitch
scan mode of SOMATOM Definition
Flash was also evaluated by Sommer et
al. in a study using an anthropomorphic
phantom and the data of 31 patients.2
The average scan time for the complete
thorax was 0.7 seconds, the average
dose 4.1 mSv, only one fifth of the dose
of a conventional gated chest scan.
Sub-mSv Heart – The robust visualiza-tion
of the coronary arteries with excel-lent
image quality at ultra low doses of
below 1 mSv was the focus of three pub-lications
by researchers from Zurich,
Switzerland3 and Erlangen, Germany.4,5
The latest study from Erlangen used the
Flash Spiral scan mode in 50 consecutive
patients with body weight up to 100 kg
and heart rates up to 60 beats per min-ute
with an average effective dose of
0.78 to 0.99 mSv and excellent image
quality.5 The average dose was 0.87
mSv. In a similar study from Zurich,
Leschka et al. found an average dose of
0.9 mSv in 35 consecutive patients.3 In
both studies 99% of all coronary seg-ments
could be evaluated3,5 and the im-age
quality was rated excellent in 94 %
of the segments or as, “at least good,” in
5 % of the segments.5
Assessment of Myocardial Perfusion –
The SOMATOM Definition Flash offers
completely new possibilities to assess
perfusion deficits in the myocardium
68 SOMATOM Sessions · May 2010 · www.siemens.com/healthcare-magazine
due to its unmatched temporal resolu-tion
and high volume coverage even at
high heart rates in stressed patients.
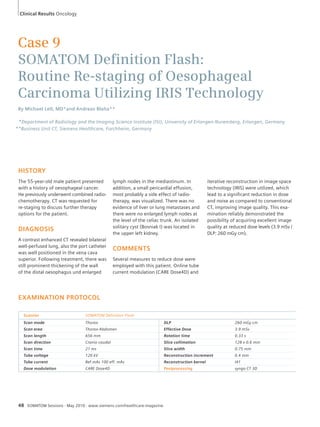
Bastarrika et al. showed that “[…] this
technique can demonstrate subendocar-dial
infarction not seen on SPECT but
confirmed by MRI and can detect isch-emia
in good correlation with stress-perfusion
MRI and SPECT.” 6 Fig. 1 shows
a short axis view of the myocardium
comparing stress perfusion measured
with the SOMATOM Definition Flash
(Fig. 1A) and SPECT (Fig. 1B).
Single Dose Dual Energy – The latest
innovation in the area of Dual Energy CT
(DECT), the Selective Photon Shield, is
based on an additional tin filter (TF)
for the high energy spectrum on the
SOMATOM Definition Flash. The Selec-tive
Photon Shield allows for the acquisi-tion
of Dual Energy data without any
dose penalty compared to standard single
energy scans and significantly improves
the separation of the energy spectra.
A group of scientists from Zurich con-firmed
this for the syngo application,
“Calculi Characterization,” using it for the
differentiation of uric acid (UA) and non-
UA stones and concluded: “DECT with TF
and 80-140 kV tube voltage settings
significantly improves the discrimination
between UA-containing and non-UA
containing urinary stones as compared
with DECT without using the TF […].”7
Lell et al. from the University of Erlangen](https://image.slidesharecdn.com/somatomsessions26int-00079316-00270153-140821164210-phpapp01/85/Somatom-sessions-26-68-320.jpg)
![Science
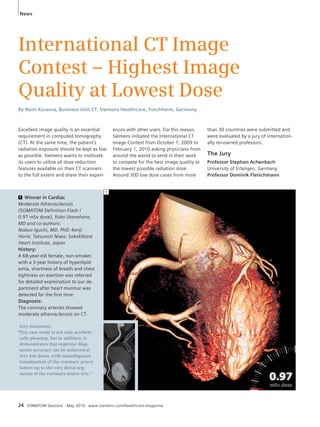
1 New frontiers in cardiac diagnosis with CT: stress-perfusion images of the heart using the unmatched temporal resolution of the
SOMATOM Definition Flash compared to SPECT. A stress perfusion scan on the SOMATOM Definition Flash nicely depicts a perfusion
defect in the myocardium (Fig. 1A). The perfusion defect could be confirmed using SPECT (arrows, Fig. 1B). Courtesy of Joseph Schoepf,
MD, Medical University of South Carolina, USA.
tages. For example, a special issue of
“Investigative Radiology” on “Advances
in CT technology,” specifically focusing
on Dual Source, Dual Energy CT and
multi-slice CT with 128 or more slices,
is scheduled for this summer.
SOMATOM Sessions · May 2010 · www.siemens.com/healthcare-magazine 69
evaluated the application of DECT to
create bone-free data sets to assess the
supraaortic arteries.8 Automatic bone
removal allows for a faster and more re-liable
diagnosis of vessels close to boney
structures. The authors conclude that
“[…] excellent bone suppression could
be achieved” using the improved scan
modes and evaluation methods on the
SOMATOM Definition Flash.
By combining multi-phase protocols to
one Dual Energy exam, the dose-saving
potential of DECT was evaluated by
Sommer et al. in patients after endovas-cular
aneurism repair using virtual non-contrast
images. They achieved a dose
reduction of 44 % compared to a bi-phase
protocol. In 70 examinations, all
24 endoleaks were detected and correctly
classified.9
More to Come – In addition to the
above mentioned publications, many
others are in the pipeline, promising to
validate the technical advancements of
the SOMATOM Definition Flash and,
even more importantly, how this trans-lates
into clinical and workflow advan-
1 Lell M, Hinkmann F, Anders K, Deak P, Kalender
WA, Uder M, Achenbach S. High-pitch electro-cardiogram-
triggered computed tomography of
the chest: initial results, Invest Radiol. 2009
Nov;44(11):728-33.
2 Sommer WH, Schenzle JC, Becker CR, Nikolaou
K, Graser A, Michalski G, Neumaier K, Reiser MF,
Johnson TR. Saving Dose in Triple-Rule-Out Com-puted
Tomography Examination Using a High-
Pitch Dual Spiral Technique. Invest Radiol. 2010
Feb;45(2):64-71.
3 Leschka S, Stolzmann P, Desbiolles L, Baumueller
S, Goetti R, Schertler T, Scheffel H, Plass A, Falk V,
Feuchtner G, Marincek B, Alkadhi H. Diagnostic
accuracy of high-pitch dual-source CT for the
assessment of coronary stenoses: first experience.
Eur Radiol. 2009 Dec;19(12):2896-903.
4 Lell M, Marwan M, Schepis T, Pflederer T, Anders
K, Flohr T, Allmendinger T, Kalender W, Ertel D,
Thierfelder C, Kuettner A, Ropers D, Daniel WG,
Achenbach S. Prospectively ECG-triggered high-pitch
spiral acquisition for coronary CT Angiogra-phy
using dual source CT: technique and initial
experience. Eur Radiol. 2009 Nov;19(11):2576-83.
5 Achenbach S, Marwan M, Ropers D, Schepis T,
Pflederer T, Anders K, Kuettner A, Daniel WG,
Uder M, Lell MM. Coronary computed tomogra-phy
angiography with a consistent dose below
1 mSv using prospectively electrocardiogram-triggered
high-pitch spiral acquisition. Eur Heart
J. 2010 Feb;31(3):340-6.
6 Bastarrika G, Ramos-Duran L, Schoepf UJ, Rosen-blum
MA, Abro JA, Brothers RL, Zubieta JL, Chia-ramida
SA, Kang DK Adenosine-stress dynamic
myocardial volume perfusion imaging with sec-ond
generation dual-source computed tomogra-phy:
Concepts and first experiences. JCCT 2010
DOI: 10.1016/j.jcct.2010.01.015.
7 Stolzmann P, Leschka S, Scheffel H, Rentsch K,
Baumüller S, Desbiolles L, Schmidt B, Marincek
B, Alkadhi H. Characterization of Urinary Stones
With Dual-Energy CT: Improved Differentiation
Using a Tin Filter. Invest Radiol. 2010 Jan;
45(1):1-6.
8 Lell M, Hinkmann F, Nkenke E, Schmidt B,
Seidensticker P, Kalender WA, Uder M, Achenbach
S. Dual energy CTA of the supraaortic arteries:
Technical improvements with a novel dual
source CT system. Eur J Radiol. 2009 Oct 8
[Epub ahead of print].
9 Sommer WH, Graser A, Becker CR, Clevert DA,
Reiser MF, Nikolaou K, Johnson TR. Image quality
of virtual noncontrast images derived from dual-energy
CT Angiography after endovascular
aneurysm repair. J Vasc Interv Radiol. 2010 Mar;
21(3):315-21.
10 Johnson TR, Schenzle JC, Sommer WH, Michalski
G, Neumaier K, Lechel U, Nikolaou K, Becker H-C,
Reiser MF. Dual energy CT: How about the dose?
Invest Radiol. 2010 (in press).
1A 1B](https://image.slidesharecdn.com/somatomsessions26int-00079316-00270153-140821164210-phpapp01/85/Somatom-sessions-26-69-320.jpg)







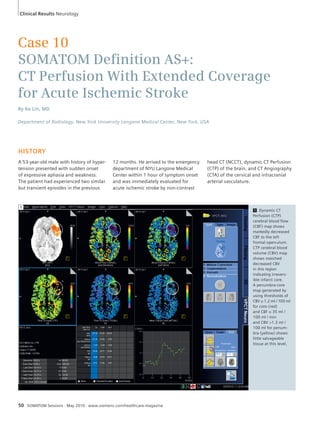
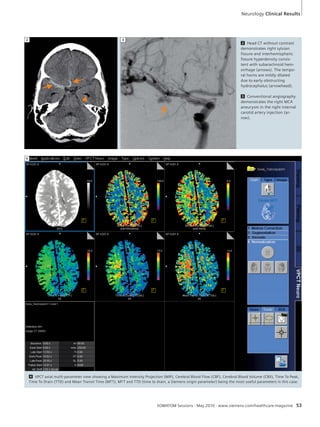
The article discusses advances in computed tomography (CT) for neuroimaging that enable both exceptional image quality and low radiation dose. It profiles Duke University Medical Center's use of Siemens CT equipment for neuroimaging. New techniques like CT perfusion, Neuro Best Contrast, and dual energy applications have changed the diagnostic approach. CT is now routinely used as the primary modality for evaluating acute neurological diseases before treatment to detect hemorrhages or other causes of symptoms like stroke. The low dose capabilities and high image quality of Siemens CT scanners are helping radiologists maximize diagnostic confidence.



























































