Download to read offline







![News
“syngo.via combines all evaluation tools in one
single workfl ow. This is a real advantage because
we need less time to evaluate all anatomic
structures relevant for the TAVI procedure.”
Tobias Pfl ederer, MD, University of Erlangen-Nuremberg, Erlangen, Germany
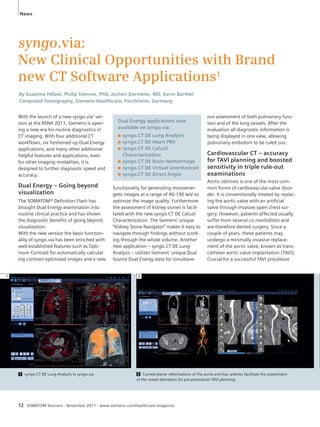
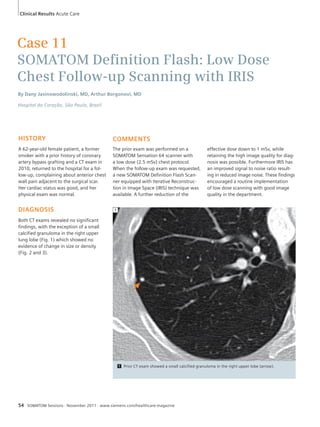
3 The automated detection of pulmonary filling defects in syngo.CT
PE CAD3 allows for a safer evaluation of triple rule-out cases.[2]
References
[1] T. Pflederer, S. Achenbach, Journal of Cardiovascular
Computed Tomography (2010) 4, 355–364
[2] Blackmon et al., European Radiology, January 2011.
4 For an evaluation of local vessel or tissue enhancement, syngo.CT Dynamic
Angio2 displays ROI-specific time attenuation curves, as well as curve and statis-tical
parameters, such as time to peak and peak enhancement.
is accurate pre-procedural planning,
where the access path for the catheter is
assessed and the optimum device type
and size are determined.
From now on, the post-processing pow-ers
of syngo.CT Vascular Analysis and
syngo.CT Cardiac Function will be com-bined
to form a dedicated workfl ow for
streamlined CT TAVI planning.
In the fi rst step of this workfl ow, the
smallest possibly detected diameter of
the iliac arteries is localized with a single
click in syngo.CT Vascular Analysis.
Quantifi cation is easily performed with
the Stenosis Measurement Tool. The
cardiologist can now determine the
optimum access route for the catheter.
Calcifi cation removal helps radiologists
to visualize calcifi cations in the entire
aorta.
An accurate assessment of the aortic
annulus is crucial for selecting the cor-rect
implant. syngo.CT Cardiac Function
displays the aortic valve plane with a
single click, allowing the short and long
axes of the aortic annulus to be mea-sured
more quickly. The length of the
device is determined by the distances of
the coronary ostia, which are obtained in
a matter of seconds. Finally, the angula-tion
for the C-arm guided intervention is
calculated and can be transferred to the
cath lab. Predicting the optimal angula-tion
with CT has been proven to help
reducing the amount of contrast agent
4
3
applied in the cath lab by 48%.[1] This
streamlined workfl ow leads to sounder
decisions in TAVI planning.
Patients exhibiting chest pain in the
emergency department often undergo a
triple rule-out examination to distinguish
between coronary artery disease, aortic
dissections, or pulmonary embolisms.
The new syngo.via version introduces
the new application syngo.CT PE CAD3
which automatically detects pulmonary
fi lling defects and which may be particu-larly
helpful if no Dual Source Dual
Energy data is available. Combined with
the CT Coronary and CT Vascular tasks,
the workfl ow CT Chest Pain + PE CAD3
boosts sensitivity[2] in challenging triple
rule-out cases. Improved automated pre-processing
in syngo.CT Coronary Analysis
is benefi cial for such cases. In addition to
the main coronaries, major coronary
branches and saphenous vein grafts are
now also automatically segmented and
labeled.
Dynamic Vessel
Evaluation redefi ned
A great step forward in terms of dynamic
vessel evaluation has been made by
introducing the new application syngo.
CT Dynamic Angio.2 For stroke patients
or patients showing transient ischemic
attack symptoms, syngo.CT Dynamic
Angio2 helps to inspect time-resolved CT
images reconstructed from dynamic
studies. It provides a temporal maximum
intensity projection (tMIP) and a tempo-ral
average volume (tAVG) for enhanced
vessel and soft tissue visualization. For
evaluating local vessel or tissue enhance-ment,
syngo.CT Dynamic Angio displays
ROI-specifi c time attenuation curves, as
well as curve and statistical parameters,
such as time to peak and peak enhance-ment.
For a phase-specifi c evaluation,
for example of the arterial or venous
phase, the Twin Slider can restrict calcu-lation
of new CT volumes to any user-defi
ned time range within the dynamic
1 syngo.via can be used as a stand-alone device or together with a variety of
syngo.via-based software options, which are medical devices
2 The information about this product is being provided for planning purposes.
The product requires 510(k) review and is not commercially available in the U.S.
3 The product is not commercially available in the U.S.](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-13-320.jpg)


![“I am typically not a big advocate of curved
planar reformations (CPR), but this work-station
actually does a really good job of
www.siemens.com/ct-cardiology
Stroke Management – Education and
Information Exchange Online
By Monika Demuth, PhD, Computed Tomography, Siemens Healthcare, Forchheim, Germany
News
SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine 17
planar reconstructions, are extremely
stable now and the results are really
good and reliable.”
Quynh Truong, MD MPH, from the
Division of Cardiology at Massachusetts
General Hospital in Boston, MA, USA,
who also helped the participants with
reading the cases, believes this course
to be a good opportunity to gain experi-ence.
Since the volume of CT scans
being performed is fairly low at some
participants’ institutions, it is important
to practice on CT and cath correlations
in order to maintain the required compe-tency
level.
One of the participants, Cristiana Scridon,
MD, from the Indian River Medical Cen-ter
in Vero Beach, Fl, USA, already
Siemens Healthcare has recently launched
a new CT stroke management online
resource for healthcare professionals.
Here, a platform is provided for introduc-ing
and discussing new diagnostic oppor-tunities
to save brain and quality of life,
synergized with information on the lat-est
Siemens CT scanners and post-pro-cessing
solutions.
After a stroke, the brain loses as many
neurons as it does in almost 3.6 years
of normal aging[1] each hour it remains
untreated. Therefore, the need for faster
diagnosis and faster treatment is central
to effective stroke management. Thanks
to a dynamic brain perfusion coverage,
Siemens Computed Tomography has
clearly improved the stroke workflow
and added value to stroke management.
The new information platform for stroke
management has been published to share
these approaches and clinical outcomes.
Peter Schramm, MD, from the certified
stroke unit at the University of Göttingen,
Germany, for example, shares his work-flow
from the arrival of a stroke patient
attended a previous CTA Academy. Her
main goal was to learn from the experts
and refresh her skills in cardiovascular
reading. With regard to syngo.via, she
states that “Practically everything works
very well and it’s very smooth. The mea-surements
go easily, and the adjustment
of the image is easy to make. So it’s great.”
Will she be coming again? – “Absolutely
every year!”
outlining the CPRs.”
Quynh Truong, MD MPH, Division of Cardiology, Massachusetts General Hospital,
Boston, MA, USA
Siemens has
launched a
CT stroke
management
website for
healthcare
professionals.
References
[1] Time is brain-quantified. Saver JL. Stroke.
2006 Jan;37(1):263-6.
in the emergency department until
the decision for further treatment. In his
institution, the door-to-needle time is
less than 20 minutes. Furthermore, lead-ing
stroke specialists share their experi-ence
and protocols in webinars and pre-sentations
on the platform. Trial versions
for Siemens latest software solutions are
available for testing developments in
stroke imaging in actual clinical practice.
This educational website was launched
to improve the knowledge of stroke
diagnosis with extended brain coverage
and is designed to integrate the experi-ences
of physicians worldwide. The online
resource can be visited via the following
link.
www.siemens.com/
CT-stroke- management](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-17-320.jpg)


![News
References
[1] May MS, Wüst W, Brand M, Stahl C, All-mendinger
T, Schmidt B, Uder M, Lell MM. Dose
reduction in abdominal computed tomography:
intraindividual comparison of image quality of
full-dose standard and half-dose iterative recon-structions
with dual-source computed tomogra-phy.
Invest Radiol. 2011 Jul; 46(7):465-70
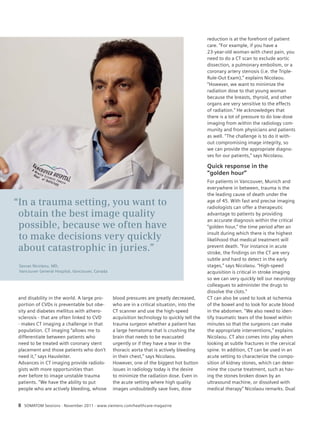
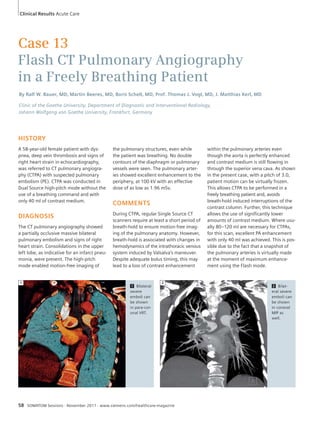
2A 2B
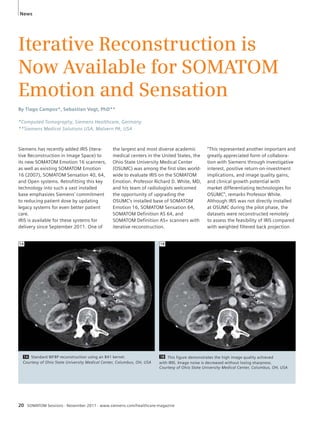
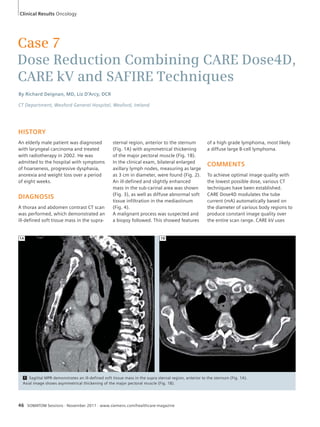
2A Standard WFBP reconstruction using a B40 kernel.
Courtesy of Ohio State University Medical Center, Columbus, OH, USA
2B This figure demonstrates the high image quality achieved with
IRIS. An improved image noise and better delineation of the liver lesion
can be achieved compared to Fig. 2A.
Courtesy of Ohio State University Medical Center, Columbus, OH, USA
SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine 21
(WFBP). Dozens of datasets were
assessed from routine examinations of
the head, thorax and abdomen. Experts
then analyzed the image quality based
on image noise, image quality, dose
effectiveness, and lesion conspicuity.
OSUMC’s team gave positive feedback in
all areas of the evaluation, highlighting
noise reduction, edge recovery, impres-sive
detail and sharpness among the
prominent benefits of IRIS. Professor
White concluded that “across the board
in this pilot project, there was unequivo-cal
gain in image quality thanks to the
application of IRIS. Artifact and noise
were consistently reduced, while low
contrast and edge definition were
enhanced, leading to improved visual-ization
of pathology. It is exciting to
realize that this can be achieved with
significant dose reduction. This is a tre-mendous
advancement!”
At the time of editorial deadline, OSUMC
were already preparing for the installa-tion
of IRIS.
The Friedrich-Alexander-University of
Erlangen-Nuremberg in Germany has
also evaluated IRIS. The university cur-rently
has a SOMATOM Definition Flash,
a SOMATOM Definition AS+, and a
SOMATOM Sensation 64. Prof. Michael
Lell, MD, was an early adopter of itera-tive
reconstruction when it was initially
released on the SOMATOM Definition
Flash in 2009, and has also worked with
the latest iterative reconstruction method
– SAFIRE1 (Sinogram Affirmed Iterative
Reconstruction). Although Prof. Michael
Lell, MD and his team were already
familiar with IRIS, the pilot study pro-vided
a good opportunity to assess its
performance against the SOMATOM
Definition systems.
Following the same approach as
OSUMC, datasets were reconstructed
remotely and compared with conven-tional
WFBP. Multiple patient datasets
were reconstructed, focusing on spe-cific
examinations, such as cardiac,
and routine examinations of the head,
thorax and abdomen. Once again,
experts rated the images based on
image noise, image quality, dose effec-tiveness,
and lesion conspicuity.
Lell and his team commented that “we
highly appreciate that iterative recon-struction,
which is fully integrated in our
clinical workflow with the SOMATOM
Definition scanners, is now available for
existing CT systems like our SOMATOM
Sensation. The excellent results with IRIS
significantly reduce dose while main-taining
image quality and lesion conspi-cuity.”[
1]
With the successful launch of IRIS for
the SOMATOM Emotion 16 (2007),
SOMATOM Sensation 40, 64, and Open,
Siemens, continues its commitment to
reducing radiation exposure for all rou-tine
CT examinations below 2.4 mSv.
“Bringing IRIS to the SOMATOM Emotion
and Sensation offers low dose to the
widest possible patient population,” says
Peter Seitz, Head of Marketing, Com-puted
Tomography, Siemens Healthcare.
1 The information about this product is being provided
for planning purposes. The product requires 510(k)
review and is not commercially available in the U.S.](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-21-320.jpg)


![News
CT Examinations Tailored Precisely
to Individual Patient Needs
Individual patient characteristics and the clinical question need to be
considered when choosing parameters and settings for a CT examination.
The latest scientifi c papers[1-4] clearly demonstrate that SOMATOM
scanners ensure CT scans are tailored to individual patient needs.
By Heidrun Endt, MD, Computed Tomography, Siemens Healthcare, Forchheim, Germany.
In the past few years, many new tech-nologies
have been introduced in
computed tomography for increasingly
automatic and individual settings of
CT scan procedures.
CARE kV – tube voltage
tailored for each examination
CARE kV is one of these new technolo-gies.
With CARE kV the tube voltage is
adjusted automatically depending on
the clinical question on a per-patient
basis. Researchers from Zurich, Switzer-land,
conducted a study for body CT
Angiography (CTA) examinations using
CARE kV on a SOMATOM Definition
AS 64.[1] In the study 40 patients were
examined and the reference setting for
the tube voltage was set to 120 kV.
CARE kV suggested the tube voltage for
each scan based on the examination
type and the topogram. This produced
the following kV settings: 80 kV
(1 patient), 100 kV (23 patients), 120 kV
(15 patients), and 140 kV (1 patient).
When changing the kV, the tube current
must also be adjusted. As CARE kV works
in combination with CARE Dose4D, this
could be achieved simultaneously and
automatically.Throughout the study
image quality was maintained, and apply-ing
CARE kV led to an overall dose reduc-tion
of 25.1% in the entire patient popu-lation,
compared to a standard 120 kV
protocol. The mean CTDIvol decreased
from 10.6 mGy to 7.9 mGy. For the
subgroup of 24 patients where the tube
voltage was reduced to either 80 kV or
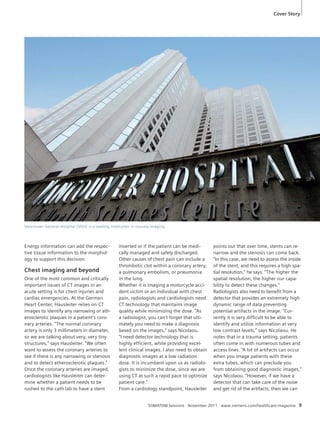
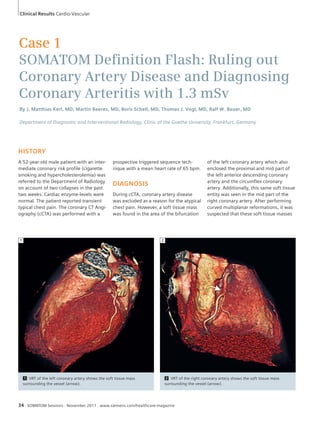
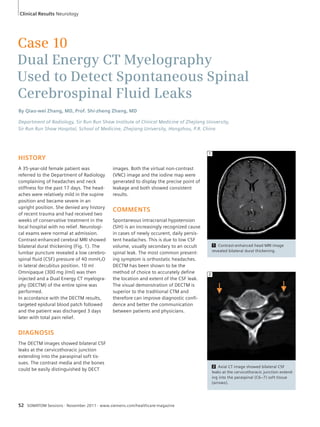
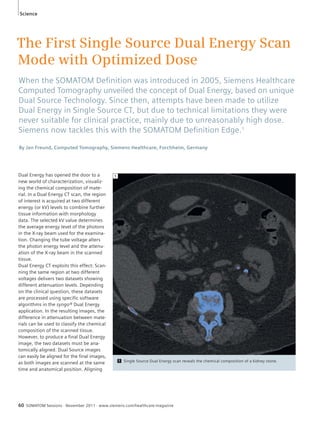
1 Fig. 1 shows a CT Angiography examination with the SOMATOM Definition AS 64 in an
82-year-old patient after endovascular aortic aneurysm repair. The scan was obtained using
CARE kV and 120 kV was chosen as reference kV setting. As the patient had a low body mass index
of 19 kg/m² CARE kV proposed 80 kV for this examination. The scan could be carried out with a
CTDIvol of 2.88 mGy and 2.7 mSv effective dose. Courtesy of University Hospital Zurich, Switzerland
1
24 SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-24-320.jpg)
![100 kV, the dose reduction was 39.3%.
The authors conclude that they “[…]
could demonstrate the beneficial effect
of this technique for body CTA […].”[1]
SAFIRE1 – designed to reduce
radiation dose for every patient
Radiation dose should always be consid-ered
when performing a CT examination,
as the benefit to potential risk ratio should
be as high as possible. Iterative recon-struction
algorithms such as IRIS and
SAFIRE1 are powerful tools for reducing
dose and following the ALARA (As Low
As Reasonably Achievable) principle. An
international group of researchers evalu-ated
the potential of SAFIRE for coronary
CTA examinations at the Medical Univer-sity
of South Carolina (MUSC).[2] In this
study 65 patients were examined with a
SOMATOM Definition Flash. The exami-nations
were obtained with the protocols
established at MUSC. The first recon-struction
used the conventional method
of filtered back projection (FBP). After-wards,
a second reconstruction with
SAFIRE was performed using data from
one tube of the Dual Source system,
corresponding to a 50% reduction
in radiation dose. When applying new
reconstruction algorithms the diag-nostic
accuracy must be taken into
account. Both reconstructions and
coronary catheter angiography exami-nations
were used for the assessment
of diagnostic accuracy.
The results show that “[...] the applica-tion
of this algorithm resulted in incre-mentally
improved diagnostic accuracy
for stenosis detection”,[2] despite the
lower dose that was used. The obese
patient population of this study had a
mean body mass index of 32.4 kg / m2.
2 Fig. 2A shows a coronary CT Angiog-raphy
examination with the SOMATOM
Definition Flash from the study conducted
at MUSC. The reconstruction was done
using FBP. For image 2B data from one
tube of the Dual Source system were
used corresponding to a 50% reduction in
dose. With SAFIRE image quality is main-tained
could be reduced allowing for a more
precise diagnosis.
Courtesy of Medical University of
South Carolina, USA
References
in Fig. 2B and blooming artifacts
[1] Winklehner A et al. Automated Attenuation-
Based Tube Potential Selection for Thoracoab-dominal
Computed Tomography Angiography:
Improved Dose Effectiveness. Invest Radiol.
2011 Jul 1. [Epub ahead of print]
[2] Moscariello A et al. Coronary CT angiography:
image quality, diagnostic accuracy, and potential
for radiation dose reduction using a novel itera-tive
image reconstruction technique-comparison
with traditional filtered back projection. Eur
Radiol. 2011 Oct;21(10):2130-8. Epub 2011
May 25.
[3] Winklehner A et al. Raw data-based iterative
reconstruction in body CTA: evaluation of radia-tion
dose saving potential. Eur Radiol. 2011 Aug
6. [Epub ahead of print]
[4] Wuest W et al. Dual source multidetector CT-angiography
before Transcatheter Aortic Valve
Implantation (TAVI) using a high-pitch spiral
acquisition mode. Eur Radiol. 2011 Aug 17.
[Epub ahead of print]
The CT scans were acquired in either ret-rospectively-
gated mode or prospectively-triggered
mode. The effective dose was
6.4 mSv for FBP, and 3.2 mSv for recon-structions
with SAFIRE. Overall, the
authors conclude that the results indi-cate
“[…] the potential for substantial
radiation dose savings […], which likely
exceed the 50% margin set forth in this
current investigation.”[2]
At the University Hospital in Zurich,[3] 25
patients underwent a body CTA exami-nation
on a SOMATOM Definition Flash.
The data were reconstructed twice: once
using FBP and once with SAFIRE. As
above, only data acquired with one of
the two tubes were analyzed for the
SAFIRE reconstructions. By comparing
two reconstructions of the examination
with different reconstruction tech-niques,
the researchers could determine
diagnostic accuracy. A key finding of the
study includes the following statement:
“In body CTA a dose reduction of >50%
might be possible when using raw data-based
iterative reconstructions, while
image quality can be maintained.”[3]
TAVI planning – less contrast
agent for multimorbid patients
Transcatheter aortic valve implantation
(TAVI) is an emerging technique and pro-vides
an alternative for patients who
need a replacement of the aortic valve
but cannot be referred to open surgery
because of other pre-existing diseases.
Whether a patient is suitable for TAVI
needs to be decided based on the anat-omy
of the aortic root and the vessels
used to gain access for the procedure.
The amount of contrast agent is an
important issue as many multimorbid
patients suffer from an impaired renal
function. An interdisciplinary group of
researchers from Erlangen examined the
potential of CT scans in 42 patients
using the high-pitch mode on the
SOMATOM Definition Flash with 40 ml
of contrast agent.[4] The mean radiation
dose for these examinations was 4.5 mSv.
The conclusion highlights the benefits:
“High-pitch spiral DSCTA [Dual Source CT
Angiography] can be used to assess the
entire aorta and iliac arteries in TAVI
candidates with a low volume of con-trast
agent while preserving diagnostic
image quality.”[4]
These scientific papers prove the bene-fits
of innovative CT technology in con-tributing
to individualized patient care.
2B
SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine 25
2A
1The information about this product is being provided
for planning purposes. The product requires 510(k)
review and is not commercially available in the U.S.](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-25-320.jpg)














![Clinical Results Oncology
Case 8
Lung Ventilation Imaging with
Dual Energy Xenon CT in Single
Breath Technique
By Prof. Norinari Honda, MD, Hisami Yanagita
Department of Radiology, Saitama Medical Center, Saitama Medical University, Kawagoe, Japan
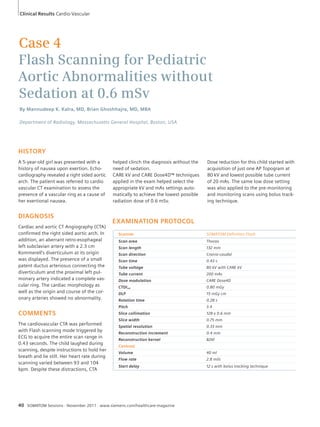
HISTORY
A 75-year-old male patient was referred
to the radiology department for detailed
imaging, after a mass was seen on his
chest radiography. He is an ex-smoker
with 53 pack years who quit two years
ago. He has been taking anti-hyperten-sive
medication for the past 20 years.
The lung auscultation sounded normal
and superficial lymph nodes were not
palpable. Focal neurological deficits
were not found. A Dual Energy xenon
ventilation CT scan using single breath
technique and a lung perfusion scintig-raphy
by SPECT examination were
ordered for detailed examination of the
lung mass and lung function. Brain MRI
was ordered to detect occult brain
metastases.
DIAGNOSIS
The lung perfusion scintigraphy and
SPECT showed a defect corresponding to
the mass. Perfusion of the other areas of
the lung was homogeneous and normal.
The ratio of the sum of the pixel counts
of the left upper lobe to that of the
whole lung was 0.86. On unenhanced
CT, the lung mass measured 6 cm at its
greatest diameter. Enlarged lymph
nodes, pleural nodules and pulmonary
nodes other than the mass were not
48 SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine
EXAMINATION PROTOCOL
Scanner
SOMATOM
Definition Flash
Scan mode Dual Energy
Scan area Thorax
Scan length 348 mm
Scan direction Cranio-caudal
Scan time 5 s
Tube voltage 80 kV / 100 kV
Tube current 190 mAs / 81 mAs
Dose modulation CARE Dose4D
CTDIvol 6.60 mGy
DLP 247 mGy cm
Rotation time 0.33 s
Slice collimation 40 x 0.6 mm
Slice width 1.5 mm
Reconstruction
0.7 mm
increment
Reconstruction
kernel
D30f
noted. Dual Energy Xenon CT showed
a ventilation defect corresponding to
the mass. And the ratio of the sum of
the pixel values of the xenon images
covering the left upper lobe to that of
the whole lung was 0.83, which was in
accordance with the scintigraphy results.
The patient was diagnosed with
T2b M0 N0 (UICC 7th edition) primary
lung cancer (poorly differentiated squa-mous
cell carcinoma) and was scheduled
for left upper lobectomy. MRI revealed
an occlusion of the right intracranial
internal carotid artery. Brain perfusion
SPECT revealed hypoperfusion of the
right frontal and parietal lobe.
COMMENTS
Xenon ventilation mapping using Dual
Energy CT single breath technique[1]
depicted the ventilation defect at the
mass and also showed normal ventila-tion
in other portions of the lungs. Risk
of peri-operative cerebral infarction was
estimated as high due to the presence
of the right carotid artery occlusion. The
patient underwent a left upper lobec-tomy.
Metastases were absent in the
intra-operative pathological examination.
Post-operative pathological analysis of
the sampled nodes revealed metastases
in one out of fourteen dissected lymph
nodes. The patient was staged as
pT2b N1 M0. He recovered uneventfully.
[1] N. Honda et al, Radiology 2011 in press](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-48-320.jpg)







![Science
SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine 61
single source scans is much more com-plicated,
and despite efforts to solve this
problem, technical limitations have pre-vented
potential solutions from being
used in clinical practice.
One suggestion for solving the difficul-ties
of aligning single source images
is to acquire two different energy levels
by changing the tube voltage several
times during one rotation. This approach
comes with several drawbacks. Firstly,
only half the number of projections or
fewer is available for each image. Sec-ondly,
this approach is only feasible at
very slow rotation speeds. These two
restrictions significantly reduce image
quality. Finally, the most crucial limita-tion
is that rapidly changing the tube
voltage requires setting the current to a
fixed value. And to penetrate large body
regions this value has to be very high.
This exposes patients to a higher dose
than necessary and is contrary to the
“ALARA (As Low As Reasonably Achiev-able)
principle. Siemens has never per-ceived
fast kV-switching as a potential
solution due to the high dose associated
with it.
A new dose optimized
technique in Single Source
Dual Energy scanning
Despite such challenges, Siemens now
introduces a dose-optimized Single
Source Dual Energy scan mode with the
SOMATOM Definition Edge, finally mak-ing
this technology accessible for a
larger number of institutions. This scan
mode consists of two consecutive spiral
scans, each acquiring a different energy
level. A scan range of 30 centimeters
can be covered with both energy levels
in 15 seconds. The first spiral scan is car-ried
out with a pitch of 0.6, followed
immediately by a spiral scan with a pitch
of 1.2 at the second energy level. Both
datasets are perfectly aligned using a
dedicated non-rigid image registration
method. To avoid doubling the dose
administered to the patient, the spirals
are set at approximately half of the total
value. Both spirals combined produce
the necessary signal level to deliver a
diagnostic Dual Energy image. With this
Single Source Dual Energy scan mode,
the entire range of dose-saving tech-niques
can be applied, including modu-lating
the tube current in real time using
CARE Dose4D™, and reducing image
noise and accordingly, radiation dose,
with SAFIRE.2
The image quality of the new Single
Source Dual Energy scan mode delivers
impressive results: A scientific study pre-sented
at this year’s RSNA demonstrates
that the image quality of Single Source
CT scans for kidney stone evaluation was
considered similar to that of the Dual
Source scans for all patients.[1] As the
study was performed using a SOMATOM
Definition AS+, not only the SOMATOM
Definition Edge benefits from the new
scan mode; the entire SOMATOM Defini-tion
AS Family can access this innovative
examination method.
The Stellar Detector detects
very low signals
Unique to the SOMATOM Definition
Edge, the Stellar Detector1 provides an
exclusive benefit: Its revolutionary
TrueSignal Technology is designed to
minimize electronic noise with the first
fully-integrated detector elements in the
industry. This makes the detector espe-cially
suitable for low-signal imaging, as
the signal-to-noise ratio is significantly
increased. With both spiral sets at much
lower dose levels than regular spirals,
this is of even greater importance, as it
increases the ability of the CT scanner
to detect very low signals. The Stellar
Detector covers an extended dynamic
range. This new feature is called
HiDynamics. It is designed to increase
the sensitivity of the detector for visual-izing
finer structures especially for the
low kV dataset.
The first Single Source Dual Energy
applications that will be available are
syngo.CT DE Calculi Characterization,
syngo.DE Gout and syngo.DE Monoener-getic2.
The characterization of kidney
stones with syngo.CT DE Calculi Charac-terization
is a good example of how
tissue characterization can support phy-sicians
in determining appropriate treat-ment.
Depending on the type of kidney
stone, treatment can vary from medica-tion
only to an invasive procedure. A
Dual Energy scan can add the tissue
information to the morphology to aid
this decision process. Gout is the most
widespread form of crystal arthropathy
and a common inflammatory joint dis-ease.
But diagnosis can prove difficult as
there are various forms of arthritis with
similar symptoms. Using syngo.DE Gout,
the disease can be detected in regions
that are often overlooked and distin-guished
from similar illnesses. Finally,
syngo.DE Monoenergetic reconstructs
images as if they were acquired at a
specific energy level between 40 keV
and 190 keV. This means that radiolo-gists
can reduce metal artifacts, such as
clamps in spine images.
Single Source Dual Energy is available
for the SOMATOM Definition AS family
and will be available for SOMATOM
Definition Edge with its release in mid-
2012.
References
[1] Leng S, et al. Renal Stone Composition Differen-tiation
using Two Consecutive CT Scans and a
Non-Rigid Registration Algorithm (abstr). In:
Radiological Society of North America scientific
assembly and annual meeting program. Oak
Brook, Ill: Radiological Society of North America,
2011
1 Under development. Not available for sale in the U.S.
2 The information about this product is being provided for planning purposes. The product requires 510(k) review and is not commercially available in the U.S.](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-61-320.jpg)
![Science
iTRIM – a New Method for
Improving Temporal Resolution in
Cardiac Computed Tomography
Iterative techniques can be used to increase temporal resolution,
a key parameter in cardiac imaging. On Siemens’ SOMATOM Perspective,1
iTRIM is used to obtain an effective temporal resolution as low as
195 milliseconds.
By Harald Schöndube, PhD*, Sebastian Vogt, PhD**, Thomas Allmendinger, PhD*, Stefan Ulzheimer, PhD*
*Computed Tomography, Siemens Healthcare, Forchheim, Germany
**Siemens Medical Solutions USA, Malvern, PA, USA
High temporal resolution is one of the
most important parameters in cardiac
imaging. Utilizing conventional cardiac
image reconstruction algorithms, the
highest achievable temporal resolution
in the isocenter of a CT image is deter-mined
by the time the scanner needs to
acquire 180º of CT projections,[1] i.e. a
half-rotation of a single source scanner.
High-end Single Source CT scanners thus
owe their good cardiac imaging perfor-mance
and high temporal resolution to
sophisticated and expensive scanner
hardware that allows the acquisition
system to be rotated faster.
As an alternative to sophisticated hard-ware
designs, image reconstruction
algorithms can be used to improve tem-poral
resolution. A long-known method
of improving the temporal resolution
in slower scanners is multi-segment
image reconstruction, utilizing data from
more than one cardiac cycle. Taking data
from up to two heart beats (bi-segment
62 SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine
approaches) is still a reasonable option
for improving temporal resolution. For
multi-segment approaches that use data
from more than two heart cycles, the
disadvantages clearly outweigh the ben-efits.
Disadvantages are a sub-optimum
dose efficiency, higher overall scan times,
and unreliable performance, since even
slight motion irregularities between
heartbeats can cause image artifacts.
Siemens has therefore developed iTRIM
(Iterative Temporal Resolution Improve-
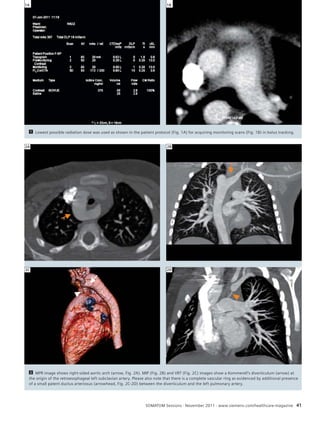
1 For each image pixel, a local histogram is generated, which is virtually
unaffected by the presence of motion artifacts and which functions as a con-straint
during the iterations in iTRIM.
N
–1000 0 HU
1](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-62-320.jpg)
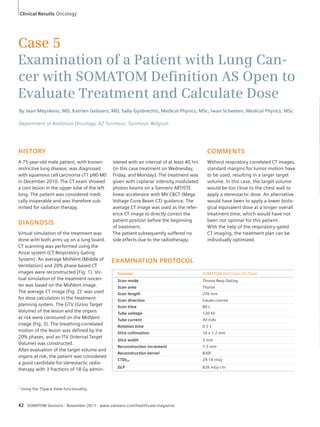
![Science
WFBP iTRIM
2 Axial images using conventional cardiac WFBP (left column) and iTRIM (right column).
The effective temporal resolution is increased by 20%, completely eliminating motion artifacts
in the right coronary artery.[4] Raw dataset courtesy of Shanghai Jiangong Hospital, Shang-hai,
SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine 63
ment Method), which is designed to fur-ther
reduce the temporal resolution of
cardiac CT images on systems not
offering the highest possible rotation
speeds.[4] This novel iterative image
reconstruction algorithm improves the
temporal resolution by 20%, effectively
reducing motion artifacts in CT images
while maintaining a very good overall
image quality and low image noise.
iTRIM is based on the observation that
the presence of motion artifacts does
not significantly change the histogram
of a CT image. This information is used
to reconstruct an image from less than
half a turn of data.[2] First, a partial car-diac
scan is performed with weighted
filtered back projection (WFBP), resulting
in a temporal resolution equivalent to
180º of CT data. For each pixel, the sys-tem
then computes a histogram within a
quadratic region centered on the pixel,
as shown in Fig. 1. An iterative recon-struction
algorithm is then started, using
only a subset of the full 180° cardiac
dataset. The size of this subset (e.g.
140°) is adapted to the target temporal
resolution. In order to expedite conver-gence,
a normal WFBP image is used as
a start image for this iterative algorithm.
The iterative loop then consists of two
steps: Firstly, the image is updated with
the projection data subset defined above
using the SART (Simultaneous Algebraic
Reconstruction Technique) iterative
reconstruction framework.[3] After each
SART iteration, an additional step is per-formed
in which the HU value of each
pixel is adjusted according to the respec-tive
histogram of the lower temporal
resolution image: Pixels with an HU
value close to a maximum of the histo-gram
are left unchanged. Pixels with an
HU value far from any maximum are
adjusted slightly towards the closest
maximum.
After the iteration has finished, a motion
detection technique is used in the final
step. The iTRIM image from the final iter-ation
of the iterative reconstruction is
combined with the conventional 180º
WFBP image. In regions that exhibit
motion, the iTRIM image is used as the
final image, whereas in static regions
the WFBP image is used.
Fig. 2 shows image examples of a car-diac
dataset, reconstructed with the typ-ical
cardiac WFBP, in direct comparison
to an iTRIM reconstruction of the same
dataset. The reduction in motion artifacts
using the iTRIM algorithm is clearly visi-ble,
while maintaining the same noise
level and overall image quality (Fig. 2).
As scientifically validated,[4] the temporal
resolution of the iTRIM reconstruction
technique can enhance the temporal res-olution
by 20%. On Siemens’ SOMATOM
Perspective1 with a rotation time of
480 ms, this yields an equivalent rota-tion
speed of 390 ms and an effective
temporal resolution of 195 ms, far
superior to the temporal resolution of
240 ms of the corresponding standard
cardiac WFBP reconstruction.
In summary, iTRIM is designed to
improve image quality in cardiac imag-
References
[1] Ohnesorge B et al. Multi-slice and Dual-source
CT in Cardiac Imaging, Springer Verlag, Berlin,
second ed. (2007).
[2] Kunze H et al. Iterative extended field of view
reconstruction, in Medical Imaging: Physics of
Medical Imaging, Hsieh J and Flynn M J (eds.),
Proc. SPIE 6510(1), 65105X (2007).
[3] Kak, AC and Slaney M Principles of Computer-ized
Tomographic Imaging, IEEE Press (1998),
(http://www.slaney.org/pct/pct-toc.html).
[4] Schöndube H et al. Evaluation of a novel CT
image reconstruction algorithm with enhanced
temporal resolution, Proc. SPIE 7961, 79611N
(2011).
People’s Republic of China
ing for systems not offering the highest
rotation speeds by providing a superior
temporal resolution compared to con-ventionally
reconstructed CT images,
while maintaining the same overall
image impression.
2A
2B
2C
2D
1 Under FDA review. Not available for sale in the U.S.](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-63-320.jpg)
![Science
Stellar Detector Performance
in Computed Tomography
The fi rst fully-integrated detector in the CT industry sets a new reference
in image quality with HiDynamics, TrueSignal and Ultra Fast Ceramics.
By Stefan Ulzheimer, PhD, Siemens Healthcare, Computed Tomography, Forchheim, Germany
Siemens has continually evolved its
technology for the most critical compo-nents
in the CT scanner, including the
X-ray tube, detector array and efficient
image reconstruction algorithms. Back
in 2002, Siemens introduced a revolu-tionary
concept for a new X-ray tube.
The STRATON® tube’s compact design
led to the development of fast rotation
speeds and Dual Source Technology.
STRATON X-ray tubes have a high power
output, small focal spot sizes and virtu-ally
no cooling delays, thanks to unique
technology that cools the anode directly.
Siemens has also improved its image
reconstruction methods continuously.
While other vendors still use single-slice
techniques which require compromises
between image quality and speed,
Siemens has developed SureViewTM for
the first generation of multi-slice detec-tors,
offering optimal dose utilization
and excellent image quality at arbitrary
pitch values. Such extensive research
and development has fueled the latest
generation of iterative reconstruction
approaches, which include IRIS, and
SAFIRE1 – Siemens´ raw-data-based
iterative reconstruction application avail-able
commercially.
High absorption, fast decay
and low afterglow
CT scanner detectors convert the attenu-ated
X-ray beam into a digital signal that
can be processed by computers. To
achieve very high dose efficiency, the
detector’s capacity for X-ray absorption
must be as high as possible. After
decades of using Xenon gas detectors in
CT, Siemens introduced the first solid-state
detector in 1999 (Fig. 1). Based on
the proprietary scintillator material,
Ultra Fast Ceramics (UFC™), the detector
offered high X-ray absorption, short
decay times, and extremely low after-glow.
The UFC layer used in Siemens CT
scanners converts almost 100% of the
X-rays into visible light, whereas Xenon
detectors can only convert between 60%
and 90% of the X-ray into a usable sig-nal.
A direct comparison of Xenon detec-tors
and UFC-based detectors indicated
an increase of 23% in dose efficiency.[1]
Decay time and afterglow are two other
important properties of scintillator
materials that characterize the light out-put
of the scintillator after the X-rays are
switched off. Decay refers to the short-term
behavior of the signal directly after
the X-ray is switched off and afterglow
is the longer-term composition of the
signal output due to luminescence. UFC
100%
Detector performance
Time
■ Siemens
Xenon
■ Siemens UFC
■ Vendor A
Xenon
Solid State
■ Vendor A
Scintillator I
Full electronic
integration
■ Vendor A
Scintillator II
Gas
1st generation 2nd generation 3rd generation
?
■
Siemens Stellar
Detector
1 First generation detectors
still used Xenon gas under high
pressure to convert the incom-ing
X-rays into electric current.
Second-generation detectors
use solid-state ceramic scintil-lators
to convert X-rays into
light, photodiodes to convert
the light into current, and
analog-to-digital converters
(ADC) to digitize the signal.
The Stellar Detector2 is the first
third-generation detector that
combines the photodiode and
the ADC in one Application-
Specific Integrated Circuit
(ASIC), dramatically reducing
electronic noise, power con-sumption,
and heat dissipation.
1
1 The information about this product is being provided for planning purposes. The product requires 510(k) review and is not commercially available in the U.S.
2 Under development. Not available for sale in the U.S.](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-64-320.jpg)
![Science
has set an industry standard with a con-sistent
decay time of 2.5 microseconds,
and an afterglow below 10-4 after 1 mil-lisecond
and 10-5 after 10 milliseconds.
Until recently, other vendors still had to
use afterglow correction mechanisms[2]
since long decay time and high after-glow
can completely ruin spatial resolu-tion.
Siemens has continued this trend
of innovation by developing the first
fully-integrated detector, which is
designed to dramatically reduce elec-tronic
noise, extend the dynamic range
and increase spatial resolution in combi-nation
with new reconstruction meth-ods.
Revolutionary new
detector design
Detector performance is not only mea-sured
by fast and high X-ray absorption,
short decay times, and low afterglow;
low electronic noise levels and a high
dynamic range are also key to designing
effective detectors. With the new Stellar
Detector,2 Siemens is pioneering the first
fully-integrated CT detector. Conventional
solid-state detectors consist of a scintilla-tor
layer that converts the incoming
X-rays into visible light, a photodiode
array that converts the visible light into
an electric current and an analog-to-digi-tal
converter (ADC) which digitizes the
signal on a separate electronic board
(Fig. 2). The number of electronic com-ponents
and relatively long conducting
paths increase power consumption, and
add to the electronic noise produced by
the detector. In the Stellar Detector,
Siemens has combined the photodiode
and the ADC in one application-specific
integrated circuit (ASIC) for the first
time in the history of CT, reducing the
path of the signal. Fig. 3A shows a
schematic of the new Stellar Detector
configuration. The light from the UFC
scintillator reaches the back-illuminated
photodiode on top of the CMOS wafer,
which houses the ADC. A digital signal
is then produced on the other side of
the wafer. This geometry consists of a
3D package of electronic circuits in a
through-silicon via (TSV); a high perfor-mance
technique for creating vertical
connections that pass completely
through the silicon wafer. Fig. 3B shows
the complete configuration of the
compact Stellar Detector array with the
ADC positioned entirely underneath the
photodiode array. This small module
replaces all the boards and electronic
components shown in Fig. 2.
Stellar Detectors transfer the digitized
signal without any losses and the elec-tronic
noise produced by the detector is
reduced by a factor of two (TrueSignal
Technology). The new ASIC consumes
85% less power and dissipates less heat,
further reducing electronic noise. Fig. 4
shows the reduced noise produced by
the new Stellar Detector compared
to a conventional second-generation
detector.
2 Prototype configuration of a second-generation detector module includes anti-scatter
collimator, scintillator layer, photodiode array and a separate electronic board with ADCs.
2
3A 3B
Light
SiO2
Back-illuminated photodiode
SiO2
Through-silicon via Fully digital signal (20 bit) 10110100101010101110
CMOS wafer (ADC)
Stud bump
Ceramics substrate
3 Schematic drawing shows the configuration of the new Stellar Detector. The light from the UFC scintillator reaches the back-illuminated pho-todiode
on top of the CMOS wafer that contains the ADC. The digital signal is then produced on the other side of the wafer (Fig. 3A). A picture of
the compact Stellar Detector array with the ADC positioned entirely underneath the photodiode array (Fig. 3B).
SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine 65](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-65-320.jpg)
![Low electronic noise and
high dynamics
In clinical CT, the attenuation of the mea-sured
object varies dramatically and so do
the signal levels at the detector. The
dynamic range describes the range of the
input signal levels that can be reliably mea-sured
simultaneously without saturation.2
HiDynamics has an exceptionally high
dynamic range of 120 dB, 15% more than
conventional detector systems, eliminating
the need to modify amplification and
avoiding detector saturation. Combined
with the noise reduction provided by
TrueSignal, Stellar Detectors can measure
smaller signals over a wider dynamic range
which directly enhances CT image quality
(Fig. 5). Applications with extremely low
signal levels at the detector benefit espe-cially
from HiDynamics and True Signal,
such as scanning large patients and low-dose
scans, as well as the low-kV datasets
of Dual Energy examinations.
Model-based and detector-optimized
reconstruction
With SAFIRE1 (Sinogram Affirmed Itera-tive
Reconstruction), Siemens introduced
the first model-based and raw data-based
iterative reconstruction application capa-ble
of reducing noise and artifacts, suited
for a broad range of applications in clini-cal
routine. SAFIRE can thus model the
Stellar Detector precisely, including the
cross talk between detector elements,
detector aperture, detector grid, and the
focal spot of the STRATON X-ray tube,
reconstructing true 0.5 mm slices and
unmatched spatial resolution in routine
clinical protocols with excellent dose effi-ciency
(Fig. 6).
SOMATOM Defi nition Edge3
and SOMATOM Defi nition Flash4
now equipped with next-genera-tion
detector technology
Siemens high-end scanners are now
equipped with the latest Stellar Detector1
in Single Source and Dual Source configu-rations.
Noise · Tube current @ 120 kV
Detector Noise Measured in a 40 cm Water Phantom
0 100 200 300 400 500
Tube current / mA
Typical 2nd generation
Detector
Stellar detector
Ideal detector without
any electronic noise
2000
1500
1000
500
0
4 Reduced noise of the new Stellar Detector3 measured with a 40 cm water phantom and
compared to a conventional second-generation detector. Stellar produces almost no electronic
noise (green line), benefiting low dose applications and large patient scans where signals are
very low.
5A 5B
5 Simulation of a hip phantom with resolution insert, conventional detector technology and
the new Stellar Detector. Using conventional technology, low signal levels in projections with
high attenuation cause streak noise patterns in clinical images (left). With the Stellar Detector
and TrueSignal Technology these unwanted noise patterns are eliminated (right).
6A 6B
6 A foot has been scanned and reconstructed with conventional technology (Fig. 6A) and
Stellar technology with optimized SAFIRE model-based reconstruction (Fig. 6B).
4
References
[1] Fuchs TOJ et al. Direct comparison of a xenon and
a solid-state CT detector system: measurements
under working conditions. IEEE Trans Med Imaging.
2000 Sep;19(9):941-8.
[2] Hsieh J, Gurmen OE, King KF. Investigation of
a solid-state detector for advanced computed
tomography. IEEE Trans Med Imaging. 2000
Sep;19(9):930-40.
Science
1 The information about this product is being provided for planning purposes.
The product requires 510(k) review and is not commercially available in the U.S.
2 Data on file.
3 Under development. Not available for sale in the U.S.
4 Under FDA review. Not available for sale in the U.S.
66 SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-66-320.jpg)
![Science
Pediatric Imaging in the Spotlight
In May 2011, more than 1000 delegates attended IPR, the “International
Paediatric Radiology Congress”. Siemens Computed Tomography highlighted
the latest innovations for individualized patient care, which were very well
received by the community.
By Heidrun Endt, MD, Computed Tomography, Siemens Healthcare, Forchheim, Germany.
Kelly Han,MD, Marylin Siegel,MD, and Michael Lell, MD,
(from left to right) presented their experiences with
the SOMATOM Definition Flash in pediatric CT imaging
during the Siemens symposium at IPR.
Marylin Siegel, MD, gave insight into CARE kV and
how the technology is applied in her institution.
References
[1] Han BK et al. Accuracy and safety of high-pitch
computed tomography imaging in young chil-dren
with complex congenital heart disease.
Am J Cardiol. 2011 May 15;107(10):1541-6.
[2] Siegel MJ et al. Radiation dose and image qual-ity
in pediatric CT: effect of technical factors and
phantom size and shape. Radiology. 2004
Nov;233(2):515-22.
[3] Lell MM et al. High-pitch spiral computed
tomography: effect on image quality and radia-tion
dose in pediatric chest computed tomogra-phy.
Invest Radiol. 2011 Feb;46(2):116-23.
SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine 67
Societies focusing on pediatric radiol-ogy
joined to organize the IPR 2011 in
London. Experts from all over the world
attended to present and discuss the lat-est
research results in the field. The con-gress
addressed all modalities relevant to
pediatric radiology, so computed tomog-raphy
was also part of the program.
Studies carried out on SOMATOM scan-ners
were covered in the scientific
sessions, and in addition, Siemens CT
presented its product portfolio on the
exhibition floor, where visitors could
view the latest technologies leading to
individualized dose management for
every patient. During the Siemens sym-posium
“SOMATOM Definition Flash:
changing paradigms in pediatric CT
imaging”, three experts in the field of
pediatric radiology reported on how
these technologies are applied in their
respective institutions.
High-pitch CT Angiography
in children
Children with congenital heart disease
were examined at the Minneapolis Heart
Institute in Minnesota, USA, Kelly Han,
MD, demonstrated how the high-pitch
mode of the SOMATOM Definition Flash
eliminates the need for general anesthe-sia
for most of the patients, and how the
dose can be lowered in these examina-tions.
One study[1] about the results has
already been published, and further
studies will follow. In addition, a very
interesting collection of cases was pre-sented
showing different anomalies and
pathologies.
CARE kV and CARE Child
Marilyn Siegel, MD, from the Mallinck-rodt
Institute of Radiology USA, sup-ported
the clinical evaluation phase of
CARE kV and CARE Child, the latest fea-tures
contributing to dose reduction in
pediatric CT imaging. In her presenta-tion,
she provided in-depth technical
background information about the
adjustment of tube voltage[2] and how
CARE kV leads to optimized tube voltage
settings for each examination, taking
the individual patient and the clinical
task into consideration. CT images from
various cases were shown, proving the
benefit that the technologies bring.
CARE Child and
Flash Spiral CT imaging
The Radiology Department of the Uni-versity
Hospital Erlangen, Germany, was
also one of the first institutions to have
access to the latest technologies. Michael
Lell, MD, presented cases scanned with
a tube voltage setting of 70 kV, which is
now possible with CARE Child. In addi-tion,
he shared his experiences with the
high-pitch mode: results of a study[3] were
presented in which even the youngest
patients could be scanned without seda-tion
or breath-hold. Information about
the workflow, scan parameter settings,
and contrast media protocols provided
a best-practice reference for this scan
mode. The symposium was very well
received, and the three presentations
clearly showed that these new technolo-gies
can benefit the youngest patients
in clinical routine.
www.ipr2011.org/](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-67-320.jpg)










![SOMATOM Sessions is also available on the internet: www.siemens.com/SOMATOM-Sessions
Note in accordance with § 33 Para.1 of the German Federal Data Protection Law:
Despatch is made using an address file which is maintained with the aid of an
automated data processing system.
SOMATOM Sessions with a total circulation of 35,000 copies is sent free of charge
to Siemens Computed Tomography customers, qualified physicians and radiology
departments throughout the world. It includes reports in the English language
on Computed Tomography: diagnostic and therapeutic methods and their applica-tion
as well as results and experience gained with corresponding systems and
solutions. It introduces from case to case new principles and procedures and dis-cusses
their clinical potential.
The statements and views of the authors in the individual contributions do not
necessarily reflect the opinion of the publisher.
The information presented in these articles and case reports is for illustration only
and is not intended to be relied upon by the reader for instruction as to the prac-tice
of medicine. Any health care practitioner reading this information is remind-ed
that they must use their own learning, training and expertise in dealing with
their individual patients. This material does not substitute for that duty and is not
intended by Siemens Medical Solutions to be used for any purpose in that regard.
The drugs and doses mentioned herein are consistent with the approval labeling
for uses and/or indications of the drug. The treating physician bears the sole
responsibility for the diagnosis and treatment of patients, including drugs and
doses prescribed in connection with such use. The Operating Instructions must
always be strictly followed when operating the CT System. The sources for the
technical data are the corresponding data sheets. Results may vary.
Partial reproduction in printed form of individual contributions is permitted, pro-vided
the customary bibliographical data such as author’s name and title of the
Imprint
contribution as well as year, issue number and pages of SOMATOM Sessions are
named, but the editors request that two copies be sent to them. The written consent
of the authors and publisher is required for the complete reprinting of an article.
We welcome your questions and comments about the editorial content of
SOMATOM Sessions. Manuscripts as well as suggestions, proposals and informa-tion
are always welcome; they are carefully examined and submitted to the edito-rial
board for attention. SOMATOM Sessions is not responsible for loss, damage,
or any other injury to unsolicited manuscripts or other materials. We reserve the
right to edit for clarity, accuracy, and space. Include your name, address, and
phone number and send to the editors, address above.
SOMATOM Sessions · November 2011 · www.siemens.com/healthcare-magazine 79
SOMATOM Sessions – IMPRINT
© 2011 by Siemens AG,
Berlin and Munich
All Rights Reserved
Publisher:
Siemens AG
Medical Solutions
Computed Tomography & Radiation Oncology
Siemensstraße 1, 91301 Forchheim, Germany
Chief Editors:
Monika Demuth, PhD
(monika.demuth@siemens.com)
Stefan Ulzheimer, PhD
(stefan.ulzheimer@siemens.com)
Clinical Editor:
Xiaoyan Chen, MD
(xiao_yan.chen@siemens.com)
Project Management: Sandra Kolb
Responsible for Contents: Peter Seitz
Editorial Board:
Xiaoyan Chen, MD, Monika Demuth, PhD,
Heidrun Endt, MD, Andreas Fischer, Tanja
Gassert, Julia Hölscher, Sandra Kolb, Axel Lorz,
Peter Seitz, Stefan Ulzheimer, PhD
Authors of this issue:
Laura Avery, MD, Massachusetts General
Hospital, Boston, MA, USA
Ralf W. Bauer, MD, Clinic of the Goethe
University, Frankfurt, Germany
Martin Beeres, MD, Clinic of the Goethe
University, Frankfurt, Germany
Arthur Borgonovi, MD, Hospital do Coração,
São Paulo, Brazil
Liz D‘Arcy, DCR, Wexford General Hospital,
Wexford, Ireland
Richard Deignan, MD, Wexford General
Hospital, Wexford, Ireland
Florian Fintelmann, MD, Massachusetts General
Hospital, Boston, MA, USA
Wang Gang, MD, Baotou Central Hospital,
Inner Mongolia, P. R. China
Katrien Geboers, MD, AZ Turnhout, Belgium
Rajiv Gupta, MD PhD, Massachusetts General
Hospital, Boston, MA, USA
Sally Gysbrechts, AZ Turnhout, Belgium
Brian Ghoshhajra, MD, MBA, Massachusetts
General Hospital, Boston, USA
Rui Juan Han, MD, Baotou Central Hospital,
Inner Mongolia, P. R. China
Prof. Norinari Honda, MD, Saitama Medical
University, Kawagoe, Japan
Dany Jasinowodolinski, MD, Hospital do
Coração, São Paulo, Brazil
Mannudeep K. Kalra, MD, Massachusetts
General Hospital, Boston, USA
J. Matthias Kerl, MD, Clinic of the Goethe
University, Frankfurt, Germany
Li Gang Li, MD, Baotou Central Hospital, Inner
Mongolia, P. R. China
Ruth Lim, MD, Massachusetts General Hospital,
Boston, MA, USA
Li Jun Ma, MD, Baotou Central Hospital, Inner
Mongolia, P. R. China
Jean Meyskens, MD, AZ Turnhout, Belgium
PD Georg Mühlenbruch, MD University Hospital
Aachen, Germany
Garrett Rowe, MD Medical University of South
Carolina, Charlston, SC, USA
Iwan Scheelen, AZ Turnhout, Belgium
Boris Schell, MD, Clinic of the Goethe
University, Frankfurt, Germany
Joseph U. Schoepf, MD, Medical University of
South Carolina, Charlston, SC, USA
Harald Seifarth, MD, Massachusetts General
Hospital, Boston, MA, USA
Kai Sun, MD, Baotou Central Hospital, Inner
Mongolia, P. R. China
Thomas J. Vogl, MD, Clinic of the Goethe
University, Frankfurt, Germany
Prof. Martin Wiesmann, MD, University Hospital
Aachen, Germany
Hisami Yanagita,Saitama Medical University,
Kawagoe, Japan
Qiao-wei Zhang, MD, Zhejiang University,
Hangzhou, P.R. China
Shi-zheng Zhang, MD, Zhejiang University,
Hangzhou, P.R. China
Tony De Lisa, external writer, Germany;
Amy K. Erickson, Medical editor, San Francisco
bay area, USA; Ingrid Horn, Scientific writer,
Germany; Eric Johnson, external journalist,
Germany; Justus Krüger, Freelance Journalist,
Hong Kong,China; Ruth Wissler, Spirit Link
Medical, Erlangen, Germany
Thomas Allmendinger, PhD; Karin Barthel;
Florian Belohlavek; Tiago Campos; Monika
Demuth, PhD; Jochen Dormeier, MD; Ivo
Driesser; Heidrun Endt, MD; Jan Freund;
Ulrike Haberland; Eri Hirayama; Susanne
Hölzer; Christianne Leidecker, PhD; Katharina
Linseisen; Bo Liu, PhD; Marion Meusel;
Katharina Otani, PhD; Harald Schöndube, PhD;
Philip Stenner, PhD; Stefan Ulzheimer, PhD;
Susanne von Vietinghoff; Sebastian Vogt;
Photo Credits:
Simon Hayter / Aurora; Stefan Sahm; Thomas
Meyer (Ostkreuz); Christian Weiss
Production and PrePress:
Norbert Moser, Kerstin Putzer,
Siemens AG, Healtchare Sector
Desing and Editorial Consulting:
Independent Medien-Design, Munich, Germany
In cooperation with Primafila AG, Zurich,
Switzerland
Managing Editor: Christa Krick
Photo Editor: Anja Kellner
Layout: Andreas Brunner, Claudia Diem,
Mathias Frisch, Melina Lopez-Ruiz
All at: Widenmayer straße 16, 80538 Munich,
Germany
The entire editorial staff here at Siemens
Healthcare extends their appreciation to all
the experts, radiologists, scholars, physicians
and technicians, who donated their time and
energy – without payment – in order to share
their expertise with the readers of SOMATOM
Sessions.
SOMATOM Sessions
$QVZHUVIRUOLIHLQRPSXWHG7RPRJUDSK
,VVXH1XPEHU-XQH
6WDQIRUG(GLWLRQ _-XQHWK²WK
Cover Story
,WHUDWLYH5HFRQVWUXFWLRQV
*RHV0DLQVWUHDP
3DJH
News
)$67$5(+LWV
WKH%XOO·V(H
3DJH
Business
VQJRYLDZLWKWKH
620$720'HÀQLWLRQ
)ODVK´$7HFKQLFDO
5HYROXWLRQµ
3DJH
Clinical
Results
1HZN93URWRFRO
(QVXUHV/RZ5DGLDWLRQ
'RVHLQ3HGLDWULF
3DWLHQWVZLWKRQJHQLWDO
+HDUW'LVHDVH
3DJH
Science
$5(N9²+RZWR2SWL
PL]H,QGLYLGXDOL]HG'RVH
3DJH
28
'LGRXPLVVRQHRIWKHSULRULVVXHV
3OHDVHYLVLWZZZVLHPHQVFRP620$7206HVVLRQVDQGRUGHURXUIUHHFRS
3OHDVHHQWHURXUEXVLQHVVDGGUHVV
,QVWLWXWLRQ
'HSDUWPHQW
)XQFWLRQ
7LWOH
1DPH
6WUHHW
3RVWDORGH
LW
6WDWH
RXQWU
HV,FRQVHQWWRWKHDERYHLQIRUPDWLRQEHLQJXVHG
IRUIXWXUHFRQWDFWUHJDUGLQJSURGXFWXSGDWHVDQGRWKHU
LPSRUWDQWQHZVIURP6LHPHQV
3OHDVHSULQWFOHDUO
Subscription
XQVXEVFULEHIURPLQIRVHUYLFH
6WDXSWRGDWHZLWKWKHODWHVWLQIRUPDWLRQ
5HJLVWHUIRU
WKHPRQWKOKHDOWKFDUHHQHZVOHWWHU
(PDLO
3OHDVHLQFOXGHPHLQRXUPDLOLQJOLVWIRUWKH
IROORZLQJ6LHPHQV+HDOWKFDUHFXVWRPHUPDJD]LQHV](https://image.slidesharecdn.com/somatomsession29-00079184-002701701-140821163646-phpapp02/85/Somatom-session-29-79-320.jpg)


The article discusses the need for fast, high-quality and low-dose CT imaging in acute care and cardiology settings when diagnosing critical injuries. Two experts, Dr. Savvas Nicolaou from Vancouver General Hospital and Dr. Jörg Hausleiter from German Heart Center Munich, emphasize the importance of CT for timely diagnosis and treatment decisions. They expect the new Stellar Detector technology to provide improved image quality while further reducing radiation dose. The detector aims to balance diagnostic image quality with low patient exposure, especially important for young patients and repeated scans. Its high spatial and temporal resolution could benefit applications like trauma, stroke and coronary imaging where seconds matter.






























































