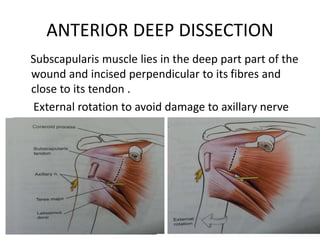
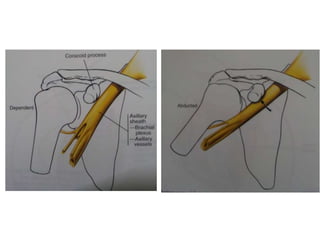
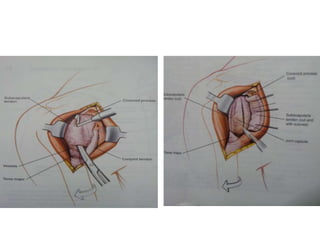
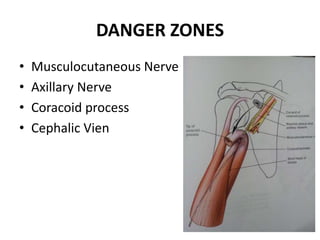
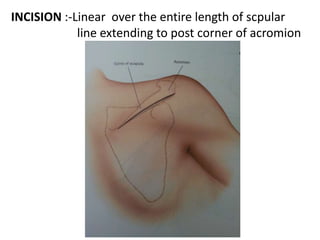
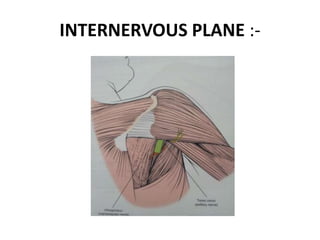
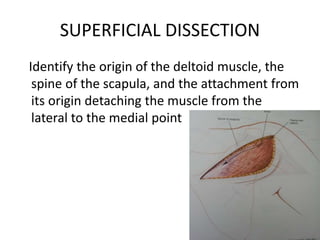
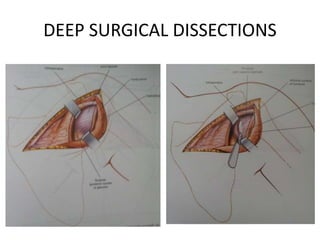
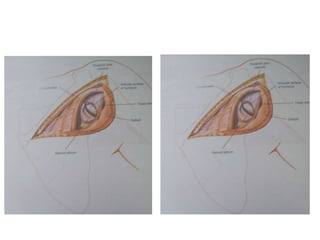
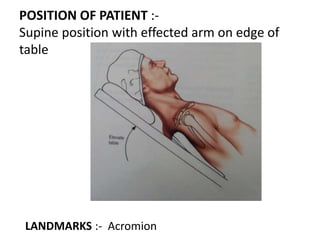
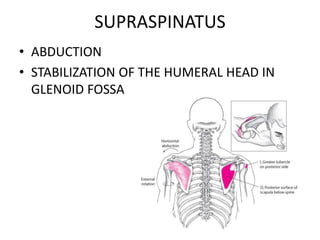
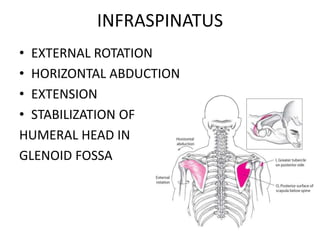
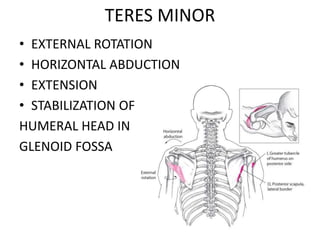
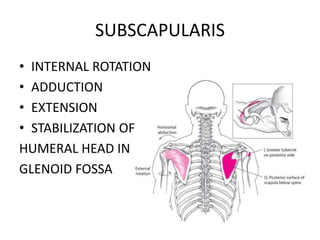
The document discusses different approaches to the shoulder joint for surgical procedures, including the anterior, posterior, and lateral approaches. It describes the indications, patient positioning, incision sites, surgical planes, and structures at risk for each approach. It also covers the rotator cuff muscles, labrum, biceps tendon, and concavity compression theory of shoulder joint stability. The concavity compression theory demonstrates that the humeral head is stabilized in the glenoid cavity by compressive forces, and this effect is increased by an intact labrum.

































![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









