Downloaded 1,557 times
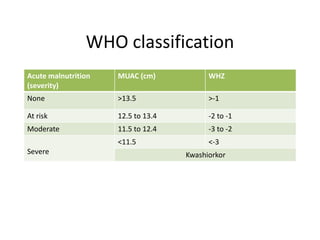
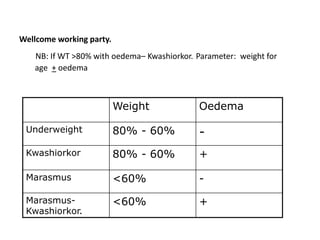


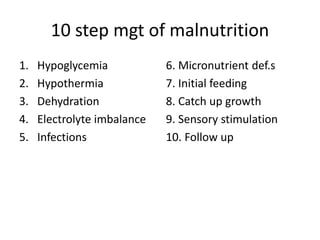
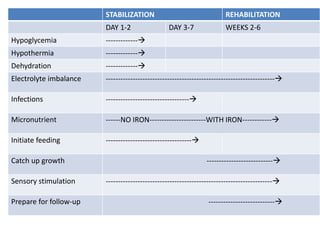
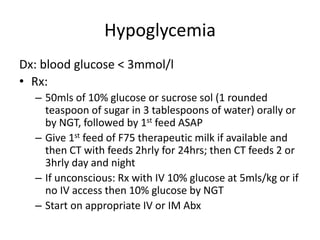

This document discusses severe acute malnutrition (SAM) in children. It begins by defining SAM and its forms, including kwashiorkor and marasmus. It then discusses the epidemiology, finding SAM contributes to over 1.5 million child deaths annually worldwide and prevalence varies significantly between developing and developed countries. Risk factors in developing countries include poverty, socioeconomic status, and infections. The document goes on to cover etiology, precipitating factors, pathogenesis of symptoms, initial assessment of children with SAM, features of kwashiorkor and marasmus, and organization of care. Children are triaged based on severity of symptoms into outpatient or inpatient treatment.










































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












