Restrictive procedures limit the amount of food that can be eaten by reducing the size of the stomach. Examples are gastric banding and sleeve gastrectomy.
What are yougoing to learn today?
• What is obesity?
• Your daily challenges
• What is obesity costing you?
• What are your surgical options?
• Summary
• What are your next steps?
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
3.
Welcome to TLCSurgery
• We are an entire practice dedicated to helping
you succeed with weight loss surgery and living
a longer, happier, healthier life!
• A multi-disciplinary Bariatric focused practice
• Lead by 2 fellowship trained, board certified Surgeons
• Nutritionists
• Psychologist
• Insurance Specialists
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
Many factors influenceobesity
OBESIT
Y
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
6.
Obesity is…
…a medical condition in which excess body fat
has accumulated to the extent that it may have
an adverse effect on health, leading to
reduced life expectancy and/or increased
health problems.
It is also…
• multi-factorial (many different factors can cause obesity)
• life-long
• progressive
• potentially life-threatening September 26, 2008
• costly
Texas Laparoscopic Consultants, LLP April 2009
7.
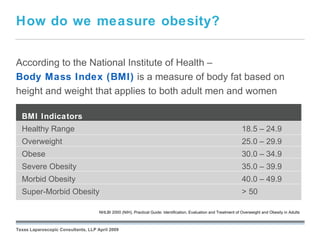
How do wemeasure obesity?
According to the National Institute of Health –
Body Mass Index (BMI) is a measure of body fat based on
height and weight that applies to both adult men and women
BMI Indicators
Healthy Range 18.5 – 24.9
Overweight 25.0 – 29.9
Obese 30.0 – 34.9
Severe Obesity 35.0 – 39.9
Morbid Obesity 40.0 – 49.9
Super-Morbid Obesity > 50
September 26, 2008
NHLBI 2000 (NIH), Practical Guide: Identification, Evaluation and Treatment of Overweight and Obesity in Adults
Texas Laparoscopic Consultants, LLP April 2009
You’re not alone
• More than 65% of adults are overweight or obese.1
• 32% of children are overweight.1
• 4.8% of adults are morbidly obese.1
• Total medical cost for obesity in 2003 was $75 billion.2
• 325,000 obesity-related deaths occur annually.3
1. Wang, Y & Beydoun, MA. Epidemiol Rev. 2007; 29: 6-28.
September 26, 2008
2. “Quick Facts: Economic and Health Burden of Chronic Disease,” CDC, updated 2007
3. Nordmann AJ et al., Arch Intern Med. 2006; 166:285-93..
Texas Laparoscopic Consultants, LLP April 2009
You face obstaclesand prejudices every
day
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
12.
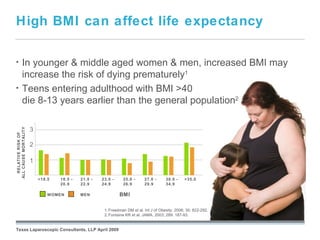
High BMI canaffect life expectancy
• In younger & middle aged women & men, increased BMI may
increase the risk of dying prematurely1
• Teens entering adulthood with BMI >40
die 8-13 years earlier than the general population2
3
ALL CAUSE MORTALITY
RELATIVE RISK OF
2
1
<18.5 18.5 - 21.0 - 23.0 - 25.0 - 27.0 - 30.0 - >35.0
20.9 22.9 24.9 26.9 29.9 34.9
WOMEN MEN BMI
September 26, 2008
1. Freedman DM et al. Int J of Obesity. 2006; 30: 822-292.
2. Fontaine KR et al. JAMA. 2003; 289: 187-93.
Texas Laparoscopic Consultants, LLP April 2009
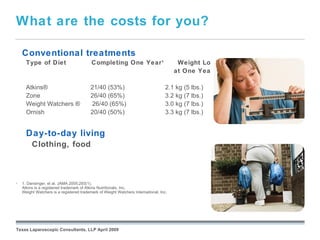
What are thecosts for you?
Conventional treatments
Type of Diet Completing One Year 1 Weight Loss
at One Year 1
Atkins® 21/40 (53%) 2.1 kg (5 lbs.)
Zone 26/40 (65%) 3.2 kg (7 lbs.)
Weight Watchers ® 26/40 (65%) 3.0 kg (7 lbs.)
Ornish 20/40 (50%) 3.3 kg (7 lbs.)
Day-to-day living
Clothing, food
• 1. Dansinger, et al. JAMA 2005;293(1).
Atkins is a registered trademark of Atkins Nutritionals, Inc.
Weight Watchers is a registered trademark of Weight Watchers International, Inc.
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
15.
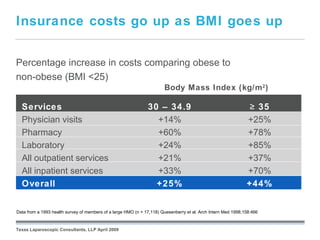
Insurance costs goup as BMI goes up
Percentage increase in costs comparing obese to
non-obese (BMI <25)
Body Mass Index (kg/m 2 )
Services 30 – 34.9 ≥ 35
Physician visits +14% +25%
Pharmacy +60% +78%
Laboratory +24% +85%
All outpatient services +21% +37%
All inpatient services +33% +70%
Overall +25% +44%
September 26, 2008
Data from a 1993 health survey of members of a large HMO (n = 17,118) Quesenberry et al. Arch Intern Med 1998;158:466
Texas Laparoscopic Consultants, LLP April 2009
Are you acandidate for weight-loss
surgery?
• BMI >35 with co-morbidities or >40 without*
• Healthy enough to undergo a major operation
• Failed attempts at medical weight loss
• Absence of drug and alcohol problems
• No uncontrolled psychological conditions
• Consensus by our multi-disciplinary team
• Understands surgery and risks
Must be dedicated to a lifestyle change
and lifetime follow-ups
September 26, 2008
*From the NIH consensus conference in 1991
Texas Laparoscopic Consultants, LLP April 2009
18.
Not all weightloss surgeries are the
same
1. Restrictive
3. Malabsorptive
5. Combination
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
19.
Restrictive Procedures
• The
size of the stomach is reduced, which limits the
amount of food patients can eat.
• The smaller stomach pouch fills quickly, helping patients
feel satisfied with less food.
• Examples of restrictive bariatric procedures:
• Gastric banding
• Sleeve gastrectomy
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
20.
Malabsorptive Procedures
• The small intestine is rerouted so that food skips a portion
of it.
• Some calories and nutrients are not absorbed.
• Currently,
surgeons rarely perform strictly malabsorptive
procedures.
• Most procedures that involve malabsorption include
restriction and are called combination procedures.
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
21.
Combination Procedures
•The surgeoncreates a small pouch, limiting the amount of food a
patient can eat.
•A section of the small intestine is rerouted, causing food to bypass
a large portion of the small intestine.
•Bypassinga portion of the small intestine means the patient’s
body absorbs fewer calories.
•Examples of combination bariatric procedures:
• Gastric bypass
• Biliopancreatic diversion with duodenal switch
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
22.
Risks of abdominalsurgery
• Bleeding
• Pain
• Shoulder pain
• Infection
• Pneumonia
• Complications due to anesthesia & medications
• Deep vein thrombosis (Blood clot)
• Pulmonary embolism (Blood clot in lung)
• Injury to stomach, esophagus, or surrounding organs
• Death
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
23.
Risks of bariatricsurgery
• Abdominal hernia • Gastrointestinal inflammation or
• Chest pain swelling
• Collapsed lung • Stoma obstruction
• Constipation or diarrhea • Stretching of the stomach
• Dehydration • Surgical procedure repeated
• Enlarged heart • Vomiting and nausea
• Gallstones, pain from passing a
gallstone, inflammation of the
gallbladder, or surgery to remove the
gallbladder
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
24.
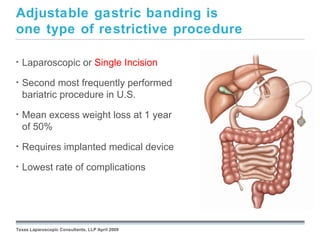
Adjustable gastric bandingis
one type of restrictive procedure
• Laparoscopic or Single Incision
• Second most frequently performed
bariatric procedure in U.S.
• Mean excess weight loss at 1 year
of 50%
• Requires implanted medical device
• Lowest rate of complications
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
What are risksand
complications of gastric banding?
• Migration of implant (band erosion, band slippage, port displacement)
• Tubing-related complications (port disconnection, tubing kinking)
• Band leak
• Port-site infection
• Esophageal spasm
• Gastroesophageal reflux disease (GERD)
• Inflammation of the esophagus or stomach
September 26, 2008
Note: Your weight, age and medical history play a significant role in determining your specific risks.
Your surgeon can inform you about your specific risks for bariatric surgery.
Texas Laparoscopic Consultants, LLP April 2009
27.
What can youexpect after
gastric banding?
Recovery takes time and patience.
• The diet is strict.
• The capacity of the stomach has changed.
• You may experience discomfort and pain as your body heals.
• Length of time to return to normal activities can vary from patient to
patient.
• Your healthcare team will advise you when to return to work and
resume prior activities.
• Lifestyle changes are necessary to ensure success.
September 26, 2008
Reference: From REALIZEband.com; life with REALIZE then recovery expectations.
Texas Laparoscopic Consultants, LLP April 2009
28.
What can youexpect after
gastric banding?
Recovery takes time and patience.
• Most patients are ready for their first adjustment after eating solid foods
for the first week. The exact timing will depend on your progress.
• If you are losing 1-2 lbs. per week you may not need an
adjustment at that time.
September 26, 2008
Reference: From REALIZEband.com; life with REALIZE then recovery expectations.
Texas Laparoscopic Consultants, LLP April 2009
29.
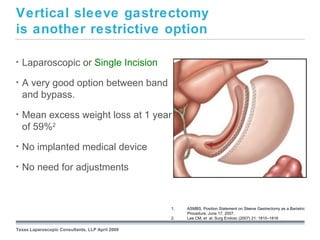
Vertical sleeve gastrectomy
isanother restrictive option
• Laparoscopic or Single Incision
• A very good option between band
and bypass.
• Mean excess weight loss at 1 year
of 59%2
• No implanted medical device
• No need for adjustments
September 26, 2008
1. ASMBS, Position Statement on Sleeve Gastrectomy as a Bariatric
Procedure. June 17, 2007.
2. Lee CM, et al. Surg Endosc (2007) 21: 1810–1816
Texas Laparoscopic Consultants, LLP April 2009
What are therisks and complications
of a vertical sleeve gastrectomy?
• Bleeding or infection
• Staple line leak
• Abdominal hernia
• Pulmonary Embolus
• Nausea and vomitting
September 26, 2008
Note: Your weight, age and medical history play a significant role in determining your specific risks.
Your surgeon can inform you about your specific risks for bariatric surgery.
Texas Laparoscopic Consultants, LLP April 2009
G
32.
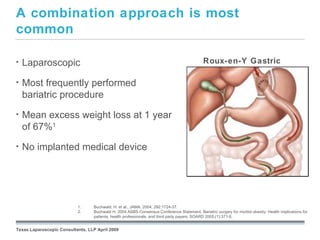
A combination approachis most
common
• Laparoscopic Roux-en-Y Gastric
Bypass
• Most frequently performed
bariatric procedure
• Mean excess weight loss at 1 year
of 67%1
• No implanted medical device
September 26, 2008
1. Buchwald, H. et al., JAMA. 2004; 292:1724-37.
2. Buchwald H. 2004 ASBS Consensus Conference Statement, Bariatric surgery for morbid obesity: Health implications for
patients, health professionals, and third party payers. SOARD 2005;(1):371-8.
Texas Laparoscopic Consultants, LLP April 2009
What are therisks and complications
of the Roux-en-Y procedure?
• Dehiscence (separation of tissue that was stitched or stapled
together)
• Leaks from staple lines
• Ulcers
• Internal hernia
• Dumping syndrome, an unpleasant side effect that may include
vomiting, nausea, weakness, sweating, faintness, and diarrhea
• Inability to detect the stomach, duodenum, and parts of the small
intestine using X-ray or endoscopy, should problems arise after
surgery such as ulcers, bleeding, or malignancy
September 26, 2008
Note: Your weight, age and medical history play a significant role in determining your specific risks.
Your surgeon can inform you about your specific risks for bariatric surgery.
Texas Laparoscopic Consultants, LLP April 2009
35.
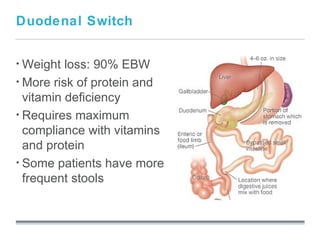
Duodenal Switch
• Weight loss: 90% EBW
• More risk of protein and
vitamin deficiency
• Requires maximum
compliance with vitamins
and protein
• Some patients have more
frequent stools
September 26, 2008
36.
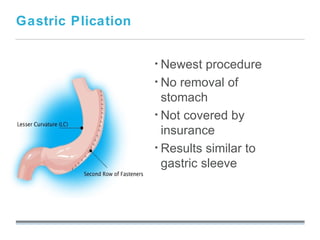
Gastric Plication
• Newest procedure
• No removal of
stomach
• Not covered by
insurance
• Results similar to
gastric sleeve
September 26, 2008
Choosing the procedurethat’s
right for you
Considerations
• Age
• Health Risk (depending on comorbidities)
• Amount of weight to lose
• Lifestyle
• Eating behaviors
Mutual decision between patient and surgeon
• Discuss with surgeon during initial consultation
• Discuss with family and friends
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
39.
Surgery can helpyou change your life
• Improves or resolves obesity-related illnesses
• Decreases mortality risk
• Reduces healthcare utilization and direct healthcare costs
Remember…surgery is a tool that requires your strong
commitment to a lifestyle change and lifetime of follow-
up
September 26, 2008
* Christou NV, Sampalis JS, Liberman M, et al. Surgery Decreases Long-Term Mortality, Morbidity, and Health Care Use in Morbidly Obese
Patients. Annals of Surgery 2004;240(3):416-424.
Texas Laparoscopic Consultants, LLP April 2009
40.
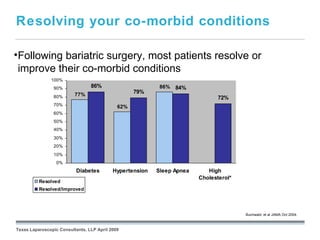
Resolving your co-morbidconditions
•Following bariatric surgery, most patients resolve or
improve their co-morbid conditions
100%
90% 86% 86% 84%
77%
79%
80% 72%
70% 62%
60%
50%
40%
30%
20%
10%
0%
Diabetes Hypertension Sleep Apnea High
Cholesterol*
Resolved
Resolved/Improved
September 26, 2008
Buchwald, et al JAMA Oct 2004.
Texas Laparoscopic Consultants, LLP April 2009
You’ve already takenthe first step
Attend seminar (Complete!)
• Obtain referral from Primary Care Physician (PCP)
• Initial consultation with surgeon
• Psychological evaluation
• Nutritional evaluation & counseling with one of our dieticians
• Verify benefits and obtain insurance authorization
• Pre-operative testing
• Surgery
• Lifelong follow-up appointments and support groups
September 26, 2008
Texas Laparoscopic Consultants, LLP April 2009
#6 Continue to speak to the patient not being alone in this challenge
#8 An opportunity to speak to the formula BMI= Weight(kg) / Height (m) 2 . Great chance to get the participants involved - create an example using the BMI wheel that has been distributed.