
Downloaded 21 times
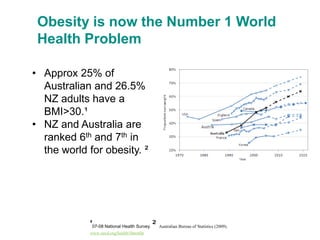
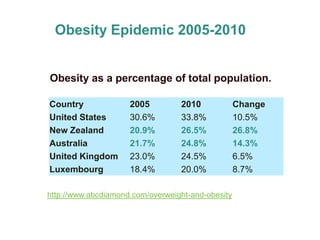
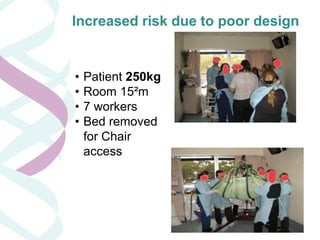

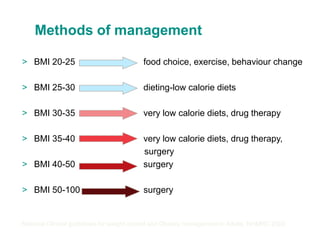
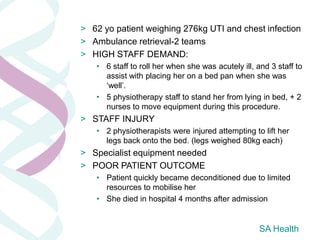

Obesity is a significant global health issue, particularly in Australia and New Zealand, where high percentages of adults are classified as obese. The document highlights the challenges and risks associated with managing bariatric patients in healthcare settings, including increased worker injury risk and longer hospital stays. It emphasizes the need for effective obesity management strategies, public health policies, and lifestyle changes to address the obesity epidemic.


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




