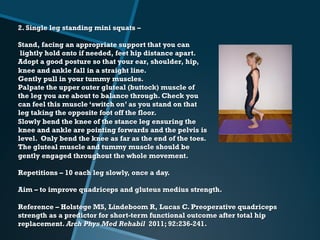
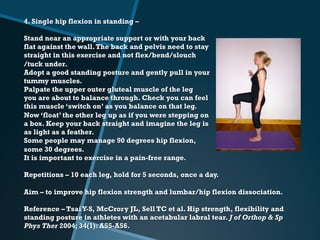
The 'HAPI' study focuses on pre-habilitation exercises designed for patients awaiting hip arthroscopy for femoro-acetabular impingement, emphasizing the need for individualized approaches in clinical settings. A range of exercises is detailed to improve strength and function in various hip muscle groups, with guidelines on technique and repetitions for effective rehabilitation. Each exercise is accompanied by references to support their efficacy and aims at enhancing patient outcomes prior to surgery.