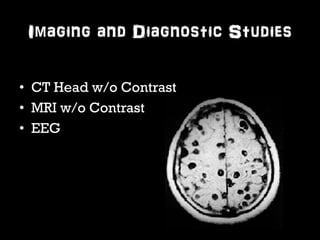
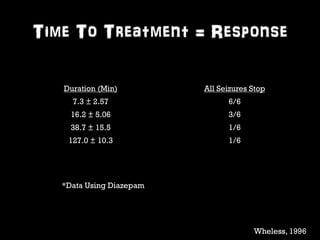
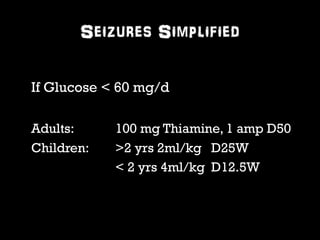
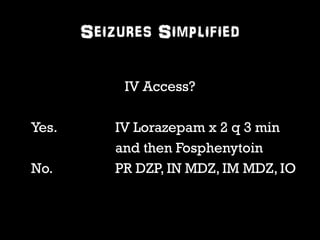
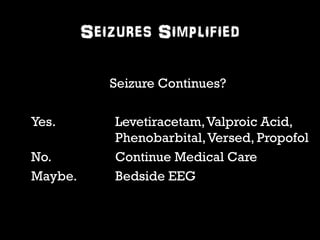
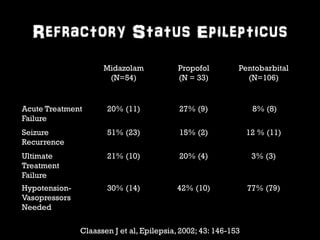
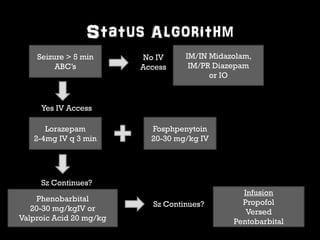
This document provides an overview of the evaluation and management of seizures. It discusses the prevalence and types of seizures, differential diagnosis, classification, assessment including history, physical exam, labs and imaging. Management of new onset seizures, abortive therapies like benzodiazepines, antiepileptic drugs, and refractory status epilepticus are covered. It emphasizes the importance of rapid treatment since time to treatment affects response, and simplifying the approach with a standardized status epilepticus management algorithm.