Download as PDF, PPTX




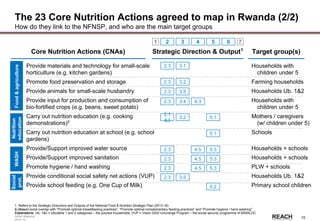
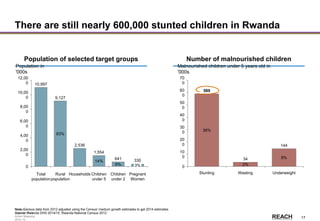
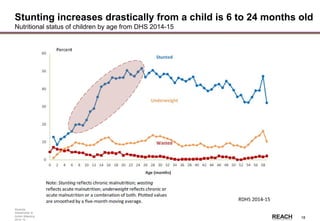
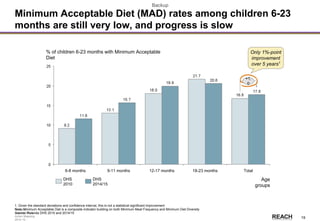
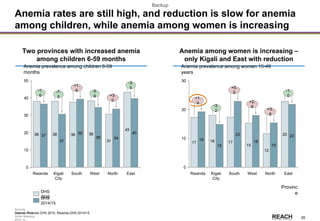
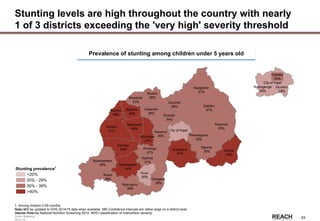
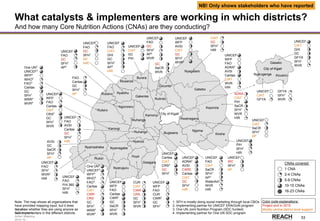
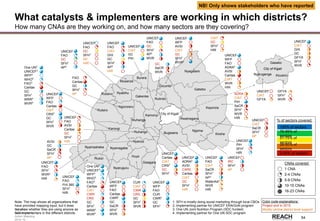
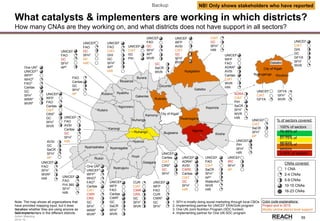

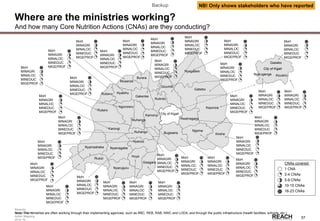



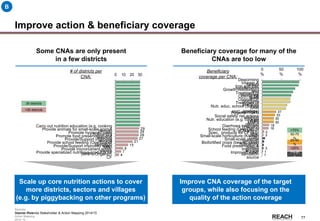
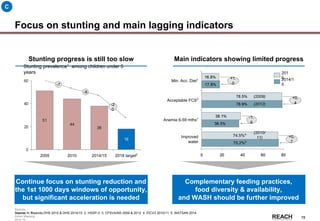
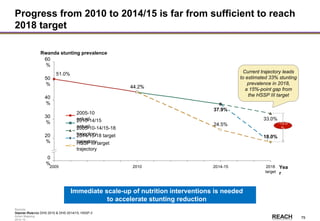
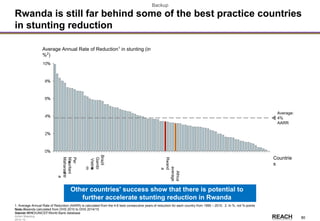

The Rwanda Stakeholder & Action Mapping report highlights the ongoing issue of chronic malnutrition, particularly stunting, which remains a significant public health concern despite some progress. It provides an overview of the key stakeholders involved in nutrition interventions, the gaps in geographical and beneficiary coverage, and emphasizes the need for further scale-up of core nutrition actions (CNAs) to enhance the effectiveness of nutrition interventions. The mapping serves as a tool for identifying partners, planning, and addressing malnutrition challenges across the country.


























































































