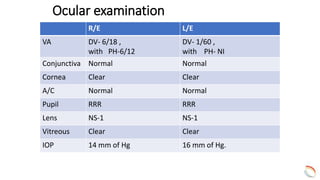
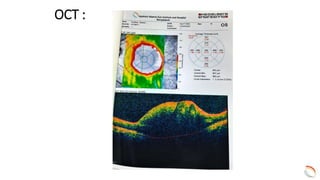
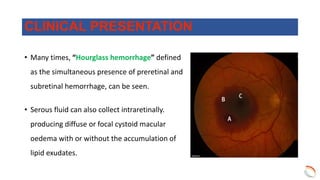
Dr. Hasan presented a case of a 60-year-old male diabetic and hypertensive patient who presented with gradual dimness of vision in his left eye over 5 days. Examination revealed a ruptured retinal artery macroaneurysm in his left eye, which was confirmed on OCT and FFA. The patient was treated with an intravitreal injection of Avastin in both eyes. At a 2-month follow-up, his vision in the left eye improved slightly but remained poor.