- The document presents a proposal on factors associated with underweight among children below 24 months in Tribeni Municipality, Bajura, Nepal.
- It outlines the background, problem statement, rationale, objectives, conceptual framework, research questions, hypotheses, methodology, and action plan of the study.
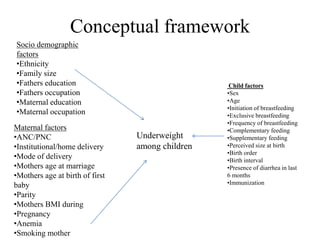
- The study aims to identify socio-demographic, maternal, and child-related factors associated with underweight in children under 2 years old in the region.





![Sample size
• Confidence interval (CI) 95% (standard value of 1.96)
• An acceptable marginal error of 7% (0.07)
• n = Z²pq/d²
• Where,
• Here, Percentage of underweight among under 5 children
according to NDHS 2016 = 27%
i.e.p=0.27
and q= 1-0.27=0.73
q = 1-p
d = (7% = 0.07)
• now, sample size( n )= 1.96²*[0.27*(1-0.27)]/0.07²
• = 155
• Non response rate = 10%
• i.e. (155*10)/100 = 15.5~16
• Now the sample size will be 155+16 =171](https://image.slidesharecdn.com/proposalpresentation-220303152221/85/Research-Proposal-Presentation-13-320.jpg)





















































![this is the Human resource M iman[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hmiman1-250914100220-640e6245-thumbnail.jpg?width=640&height=640&fit=bounds)




























