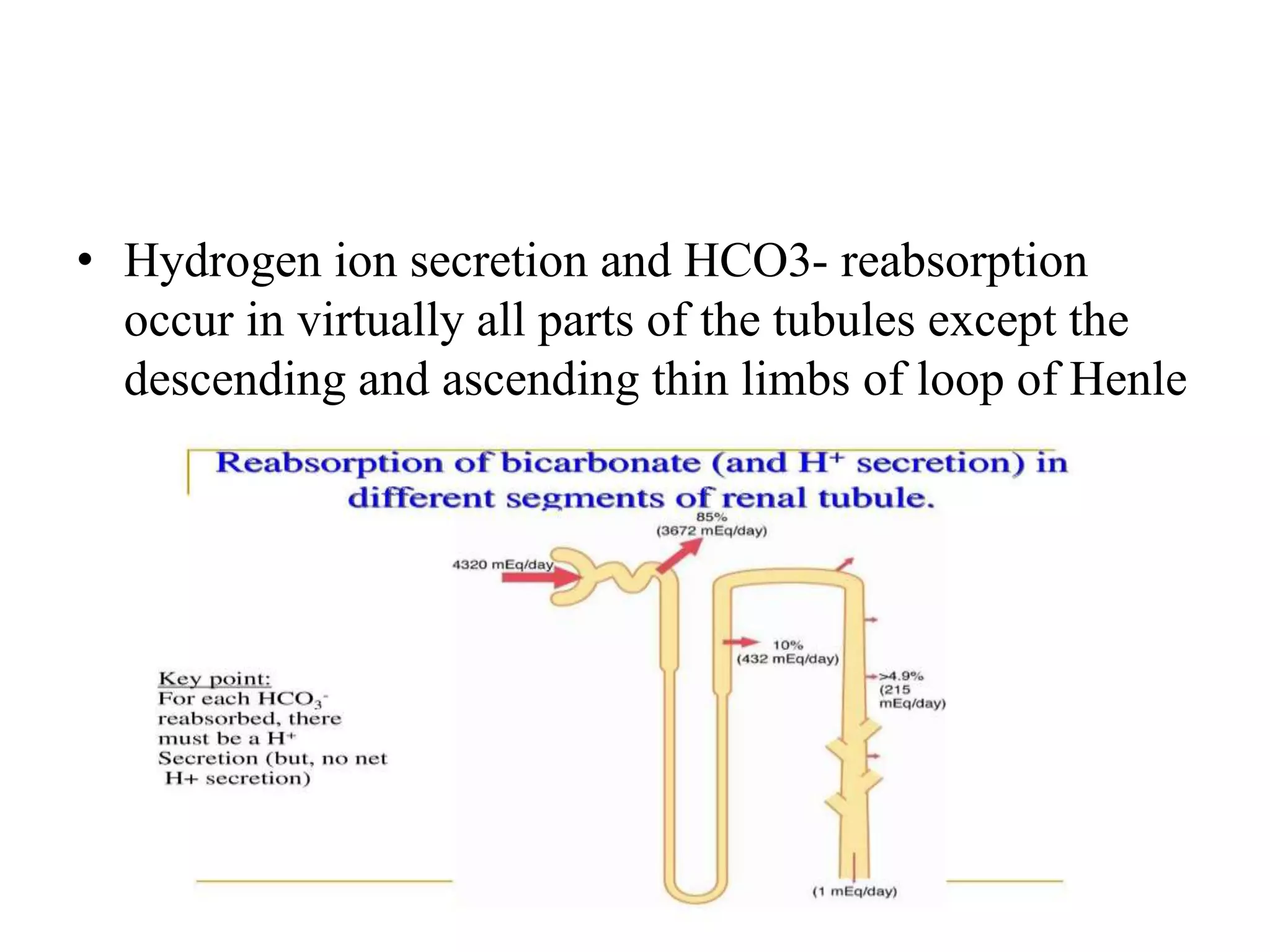
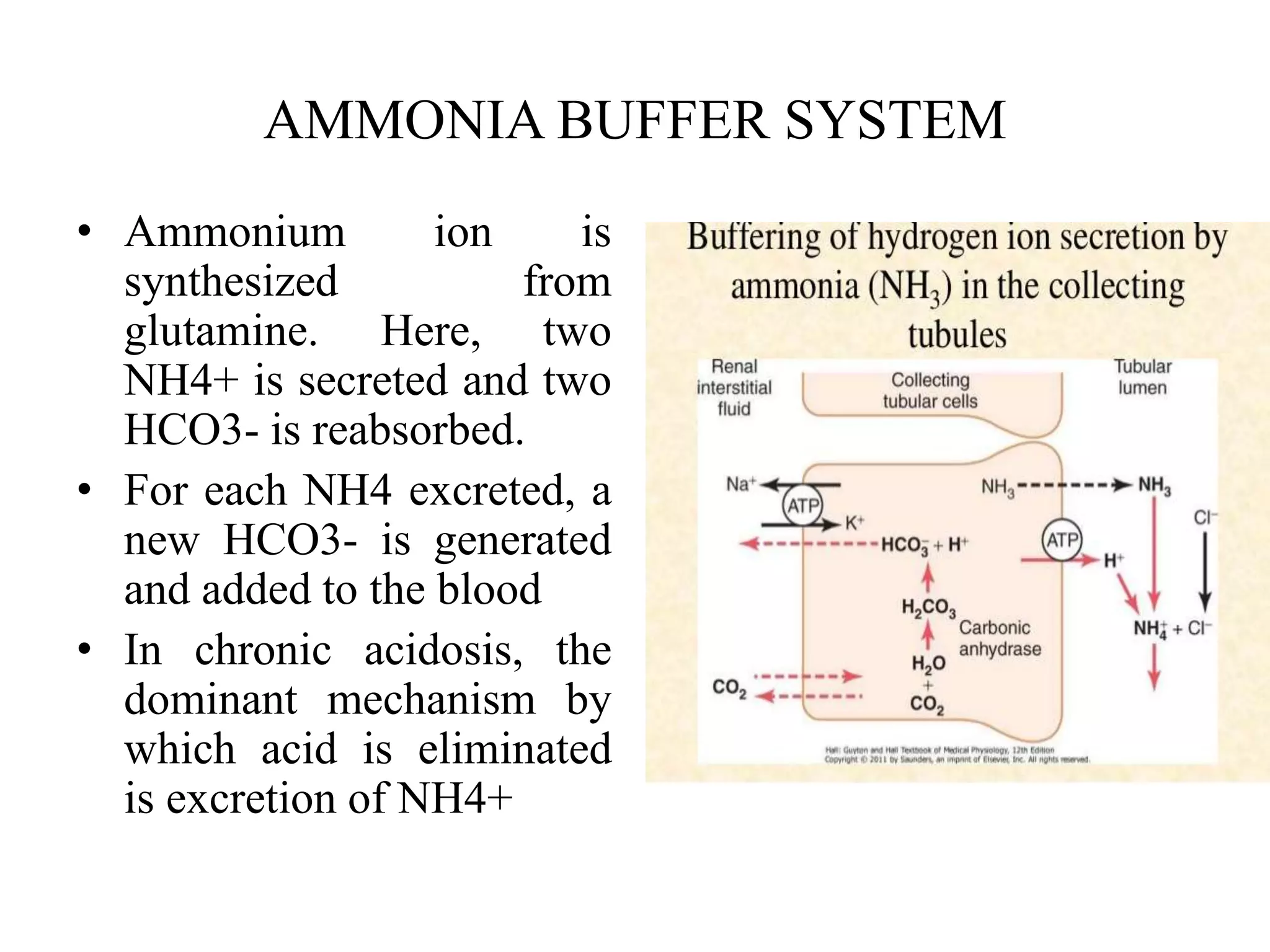
The kidneys play a key role in maintaining acid-base balance by secreting hydrogen ions into the urine and reabsorbing bicarbonate from filtered blood. There are three main mechanisms: 1) secretion of hydrogen ions via sodium-hydrogen countertransport in the proximal tubule and loop of Henle, 2) reabsorption of filtered bicarbonate by converting it to carbonic acid which enters tubular cells and reforms bicarbonate, and 3) secretion of hydrogen ions directly via proton pumps in collecting duct intercalated cells. Excess hydrogen ions that are not bound to bicarbonate instead react with phosphate and ammonia buffers to form compounds that are excreted in urine, generating new b




![• Because H+ concentration normally is low, and
because these small numbers are cumbersome, it is
customary to express H+ concentration on a
logarithm scale, using pH units. pH is related to the
actual H+ concentration by the following formula
(H+ concentration is expressed in equivalents per
liter)
• pH= -log [0.00000004]
• pH= 7.4](https://image.slidesharecdn.com/renalacidbase-230925023650-cec32f05/75/renal-acid-base-pptx-6-2048.jpg)