Download as PDF, PPTX

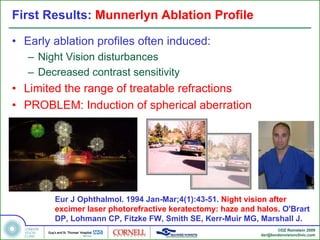
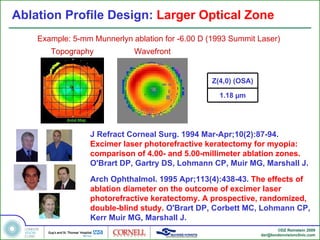
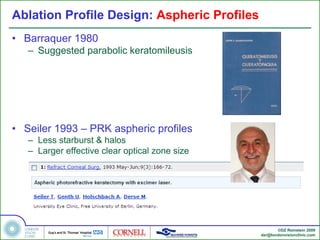
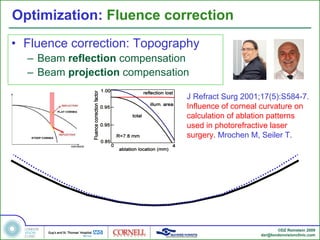
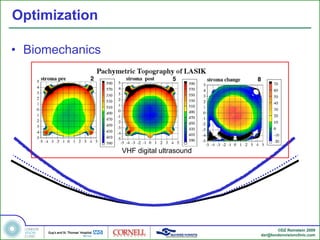
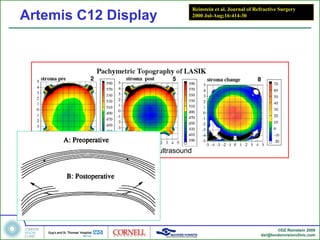
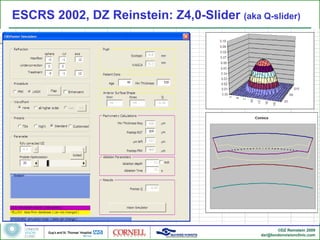
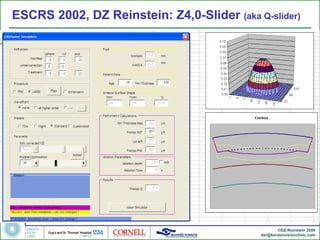
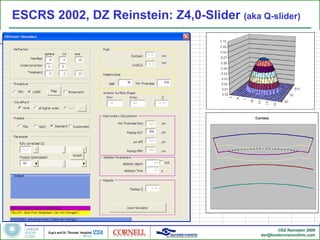
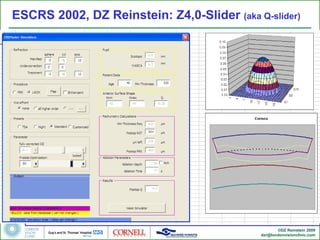
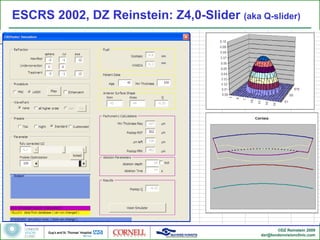
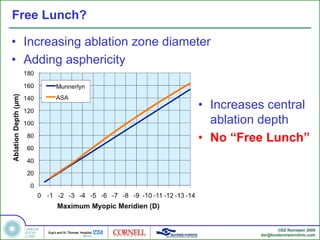
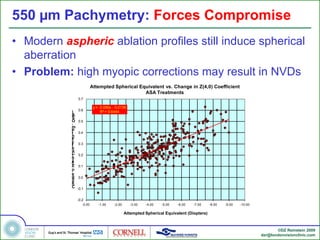
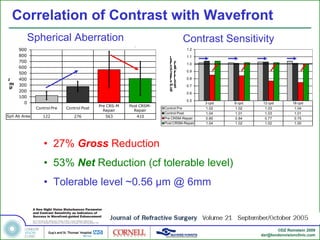
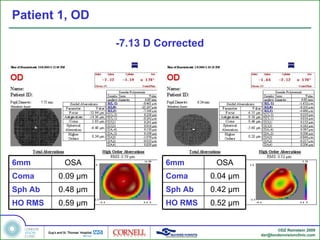
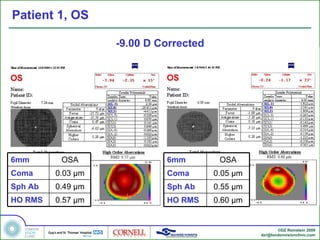
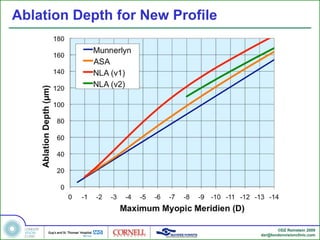
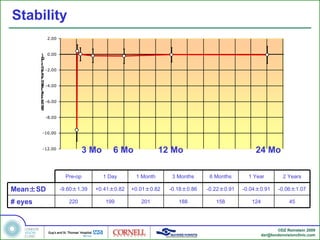

This document discusses the development of laser-assisted in situ keratomileusis (LASIK) ablation profiles for treating high myopia. Early profiles caused problems like increased spherical aberration and night vision disturbances when treating higher refractive errors. Researchers optimized profiles by using larger optical zones, incorporating aspheric designs, and accounting for biomechanical factors. However, high corrections still induced spherical aberration due to limits of corneal thickness. Wavefront-guided LASIK was explored as a method to treat spherical aberration induced by ablation.










































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

