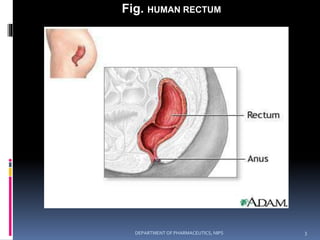
The document discusses rectal drug delivery systems. It provides a brief history of rectal medications dating back to ancient civilizations. It describes the anatomy and physiology of the human rectum, noting its length, pH, blood supply, and limited surface area available for drug absorption. Several advantages and disadvantages of the rectal route are outlined. Factors affecting drug absorption from the rectum include physiological factors of the drug and rectum as well as physicochemical properties of the drug. Common rectal dosage forms include creams, ointments, suppositories, solutions, and suspensions. The document discusses these forms in detail and provides examples of commercial rectal products.



![@
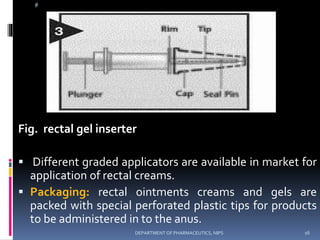
PACKAGING: Packaging is done after lubrication with
proper lubricant in aluminum foil or in other suitable
material. And with indication
[ STORE IN A COOL PLACE ]
The use of gels, foams or ointments for rectal
administration can afford advantages over liquid
formulations because retention of the dosage form in the
rectal cavity reduces patient compliance problems. Drug
release with semisolid dosage forms is usually limited to
local indications such as hemorrhoids and lower bowel
inflammation (proctitis). Drug release and subsequent
pharmacologic action is usually faster with semisolid
formulations than with solid suppositories since a lag
time is not required for melting or dissolution.
22DEPARTMENT OF PHARMACEUTICS, NIPS](https://image.slidesharecdn.com/rectaldds-160404045704/85/Rectal-dds-22-320.jpg)






























![Rectal drug delivery system [RDDS]](https://cdn.slidesharecdn.com/ss_thumbnails/rectaldrugdeliverysystemrdds-160619063853-thumbnail.jpg?width=640&height=640&fit=bounds)













































































