Downloaded 45 times
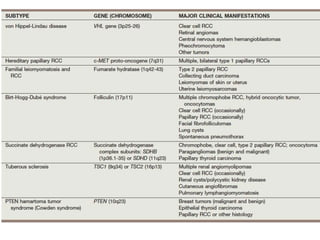

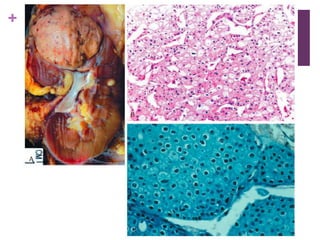


This document summarizes renal cell carcinoma (RCC), including its incidence, risk factors, pathology, subtypes, clinical presentation, and prognosis. RCC accounts for 2-3% of adult cancers and is the most lethal urologic cancer. Clear cell RCC is the most common subtype, accounting for 70-80% of cases. Other subtypes include papillary RCC, chromophobe RCC, collecting duct carcinoma, and unclassified RCC. Tumor size, grade, stage, and histologic subtype are important prognostic factors. Over 60% of RCCs are now detected incidentally with improved imaging techniques.






























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















