Download to read offline




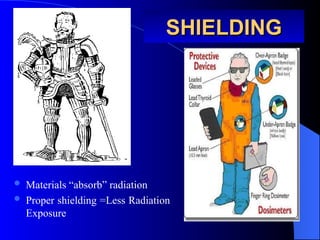

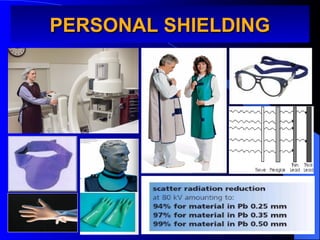
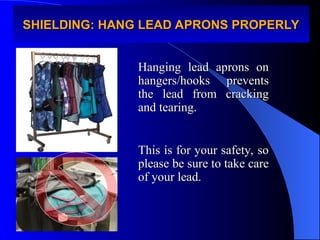


The document outlines the risks and safety measures related to radiation exposure for practicing anesthesiologists, emphasizing the importance of understanding radiation characteristics, biological effects, and safety protocols. It highlights the significant occupational radiation exposure anesthesiologists face, especially during fluoroscopic procedures, and stresses the need for education on radiation safety practices and personal monitoring. Recommendations include adhering to the ALARA principle, utilizing protective equipment, and continuously updating knowledge on radiation protection.












































































