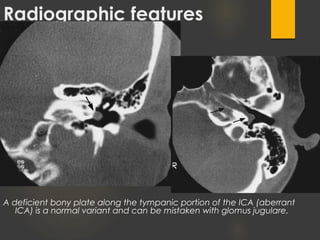
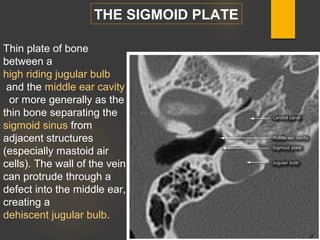
Tinnitus is the perception of sound when no external sound is present. It can be subjective, heard only by the patient, or objective, able to be heard by an examiner. Pulsatile tinnitus is a rhythmic type of tinnitus that is synchronous with the heartbeat. Imaging findings associated with pulsatile tinnitus include aberrant internal carotid arteries, persistent stapedial arteries, high or dehiscent jugular bulbs, sigmoid sinus wall anomalies, and vascular tumors or malformations. A detailed history, physical exam, audiologic evaluation, and imaging are needed to evaluate tinnitus and identify potential underlying causes.