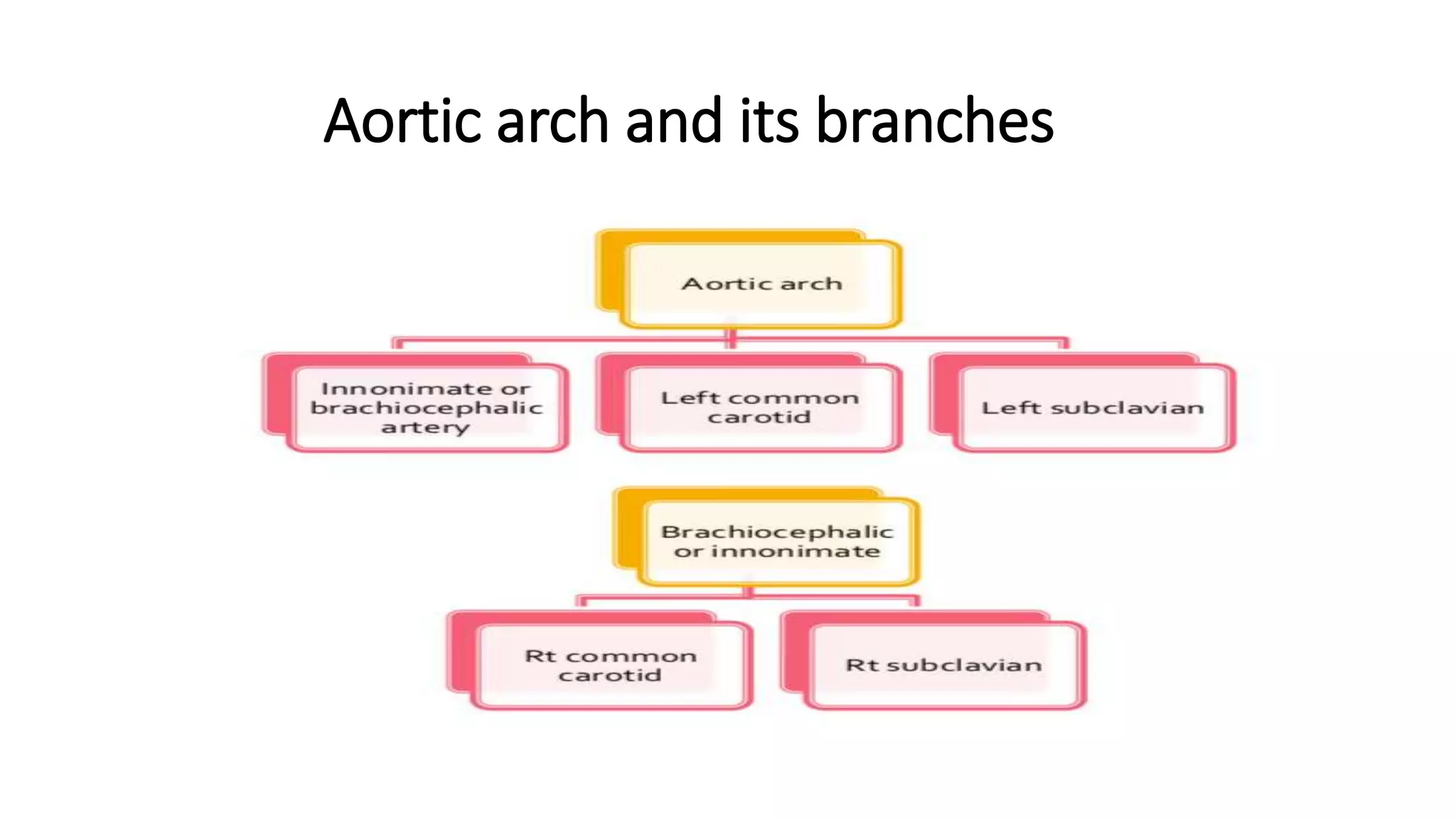
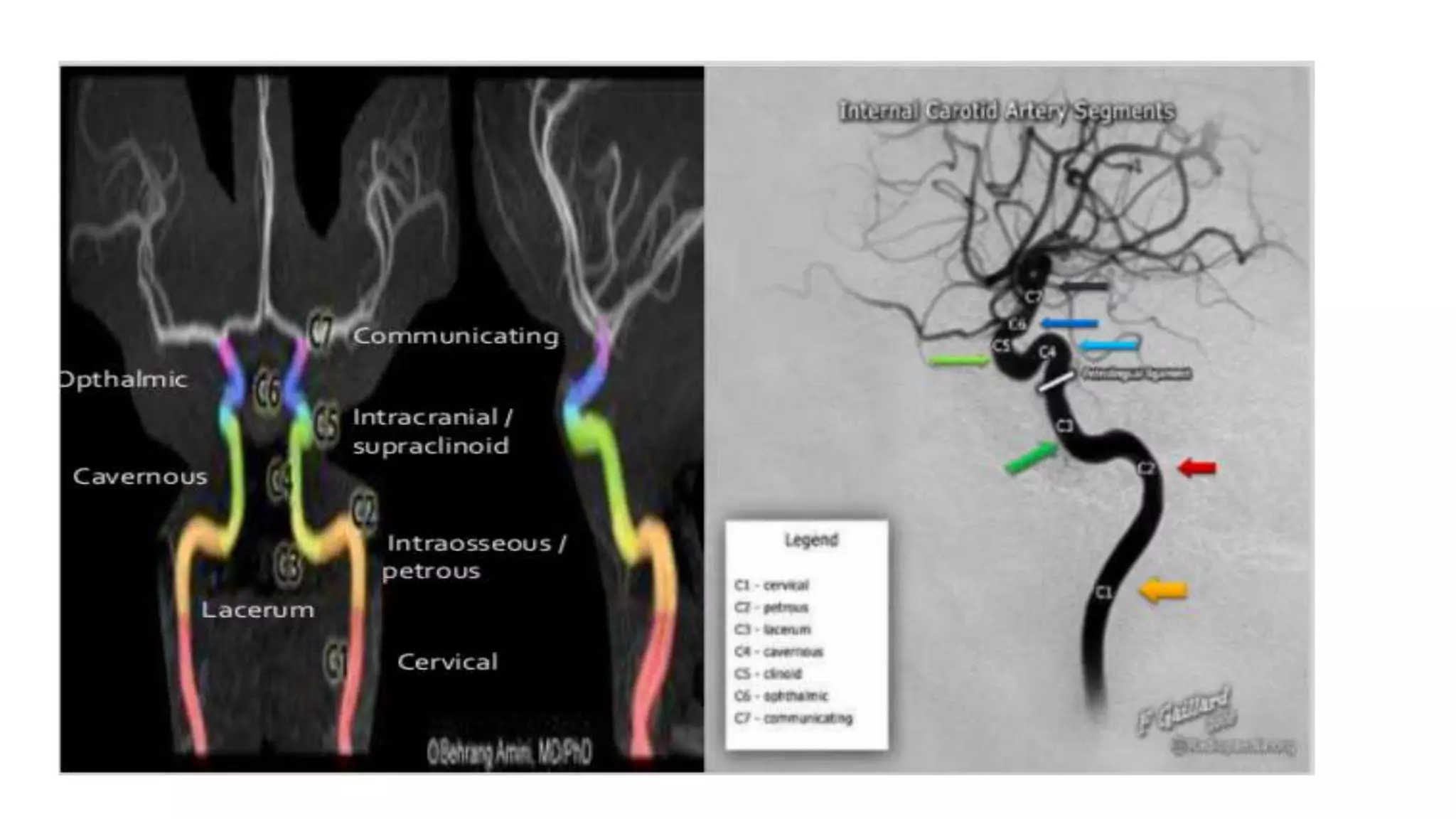
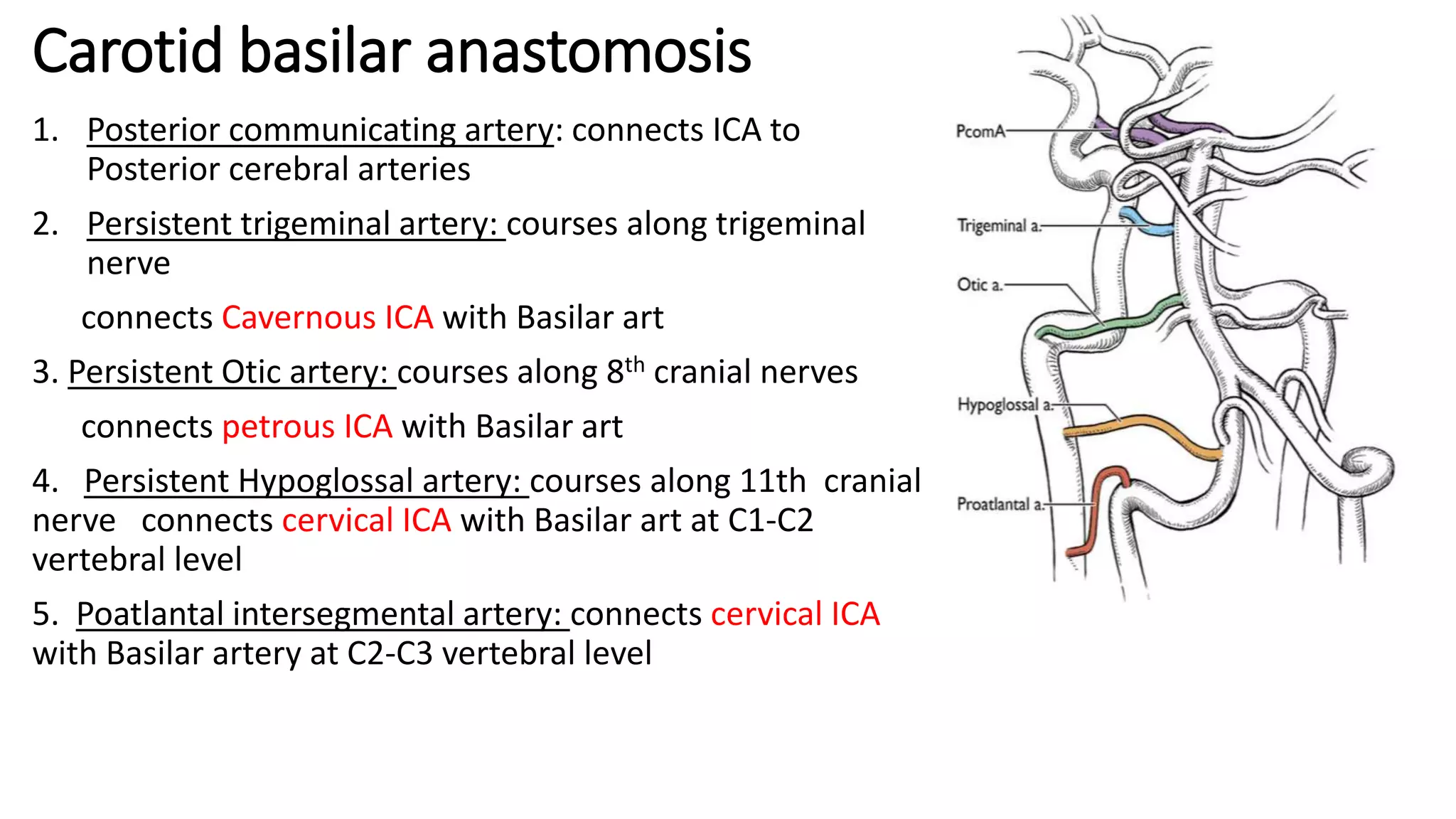
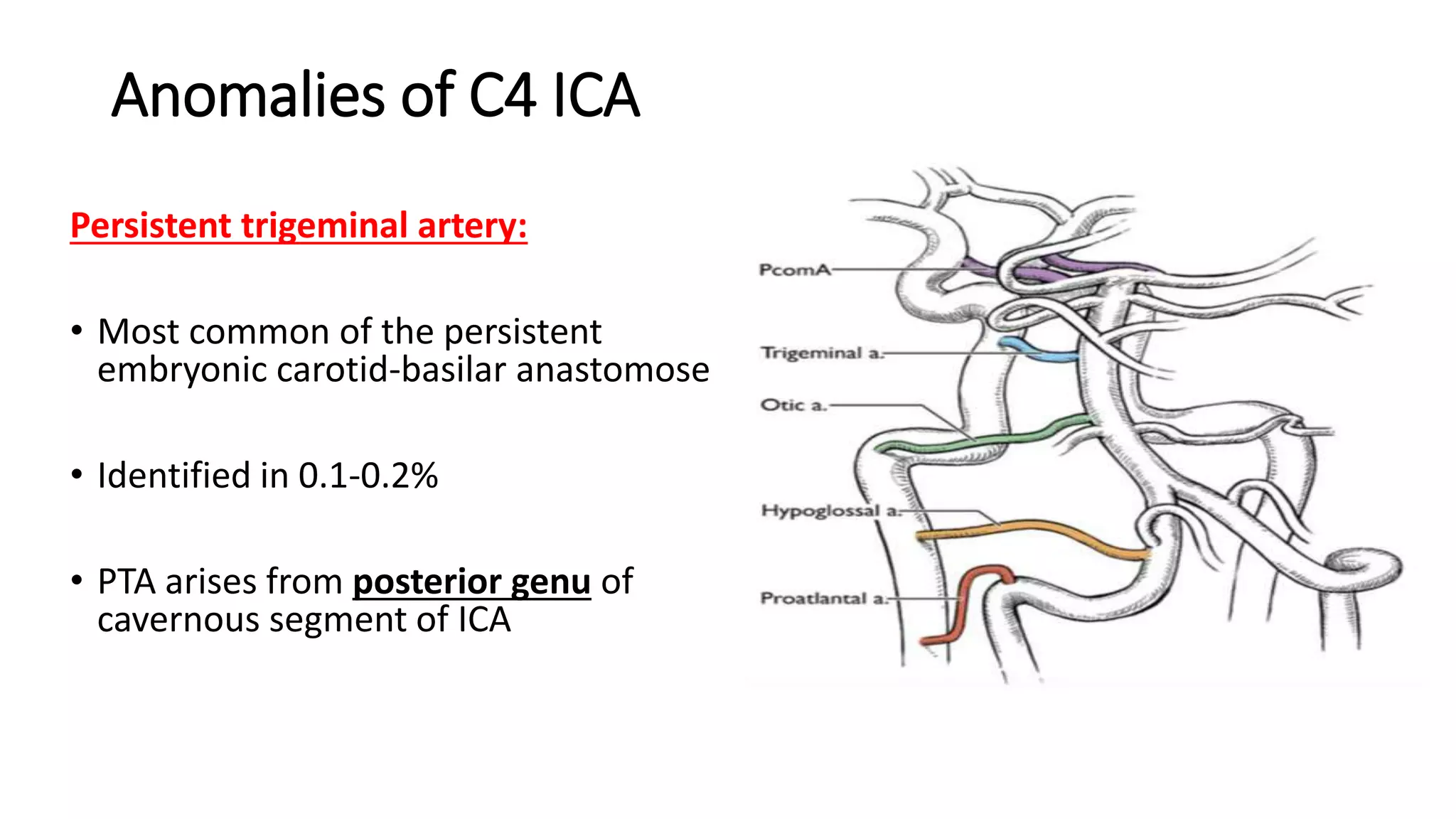
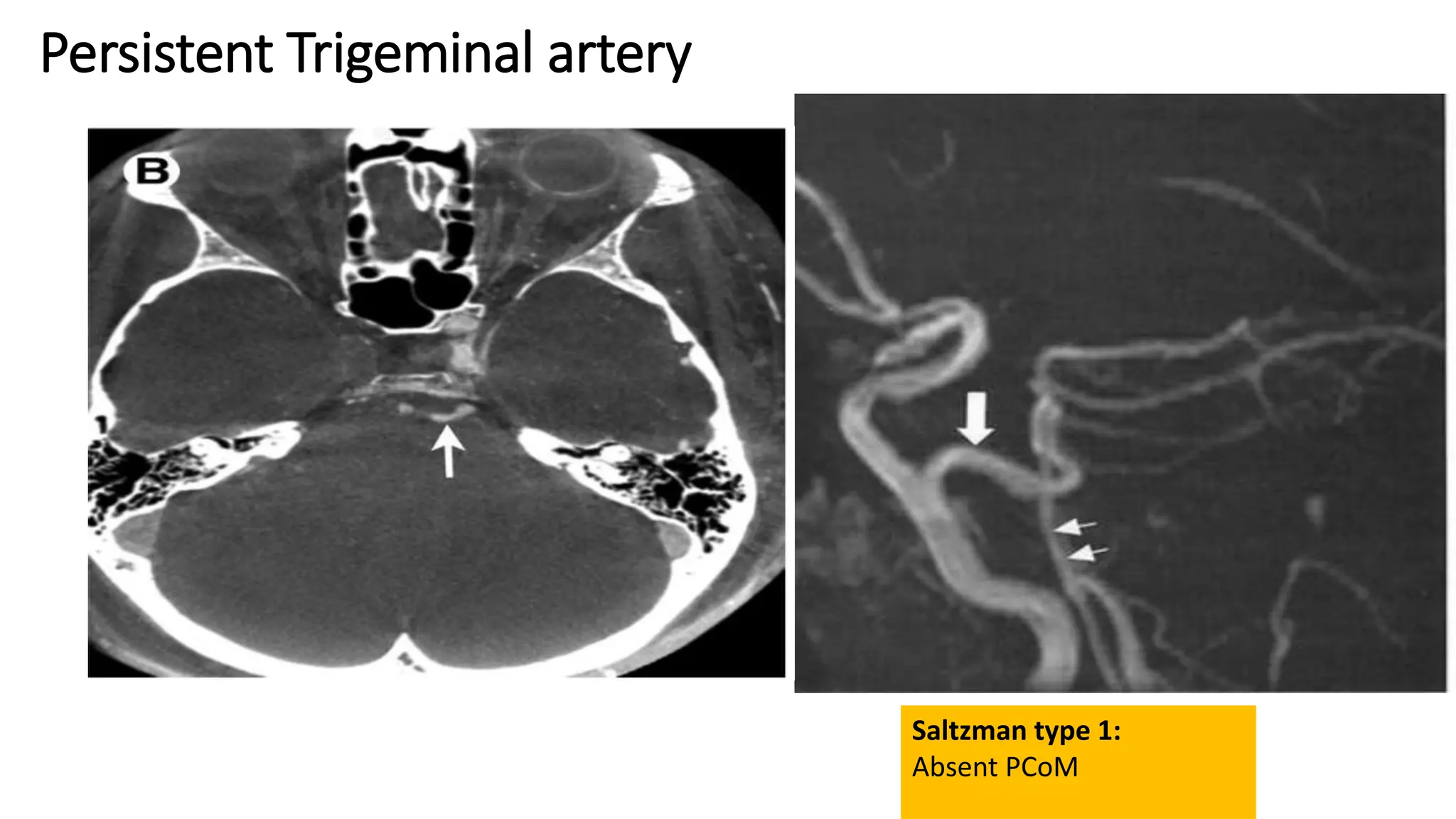
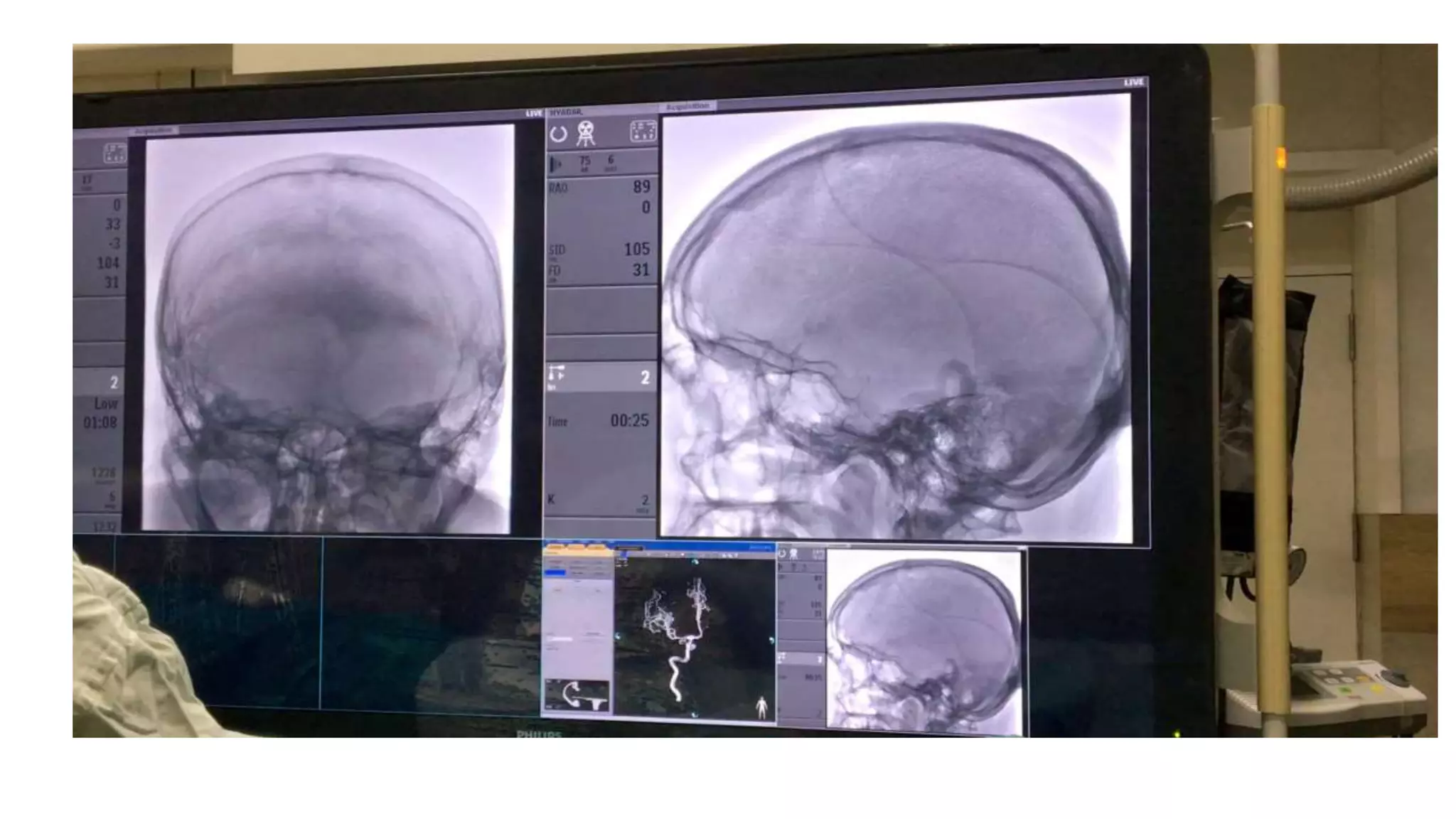
This document provides an overview of angiography and the course of blood vessels supplying the brain. It describes the aortic arch and its branches, as well as the internal carotid artery in detail. The internal carotid artery is discussed in segments from the cervical segment through the cavernous segment. Common variants and anomalies are described for various segments including the persistent trigeminal artery originating from the cavernous segment of the internal carotid artery.








































































































![Vascular anatomy of head, [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/vascularanatomyofheadautosaved-181218123734-thumbnail.jpg?width=640&height=640&fit=bounds)




































