Downloaded 212 times

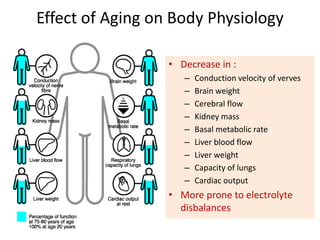
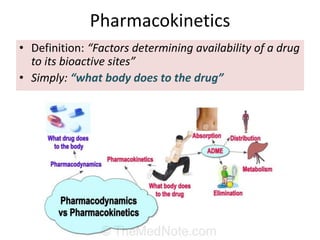
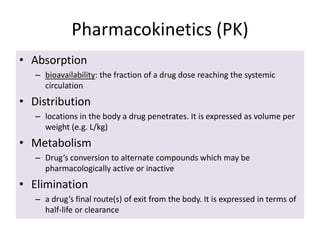
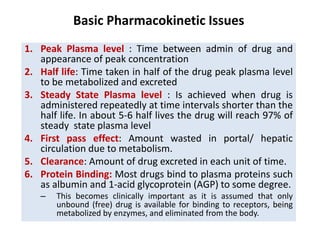
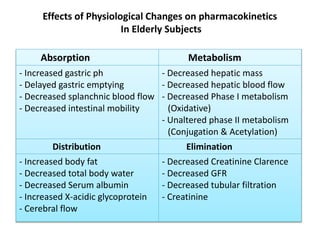
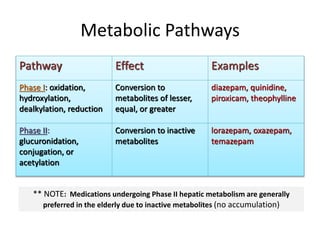
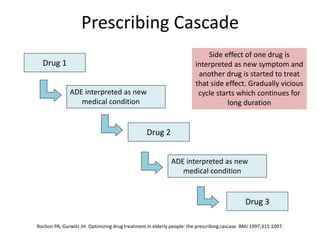
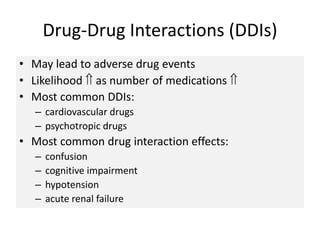
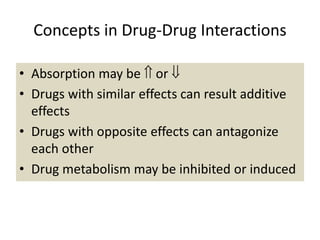
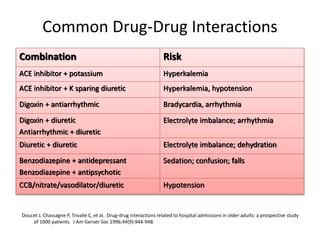
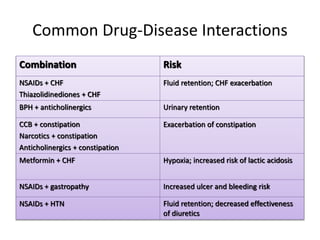
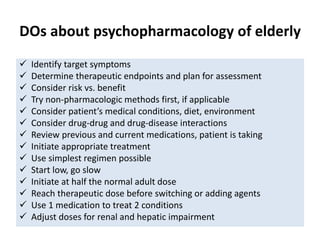
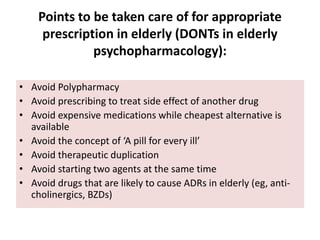


The document outlines key principles in geriatric pharmacotherapy, focusing on the impact of aging on pharmacokinetics and pharmacodynamics, as well as the various challenges faced, such as polypharmacy and adverse drug events (ADEs). It emphasizes the importance of careful prescribing practices, including starting low doses and considering non-pharmacologic therapies to mitigate risks. Additionally, strategies to prevent polypharmacy and enhance medication adherence in elderly patients are discussed, highlighting the need for regular medication reviews and education.











































































































