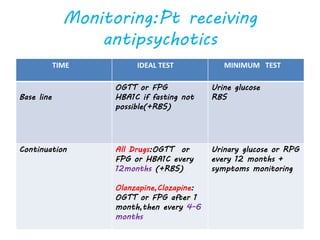
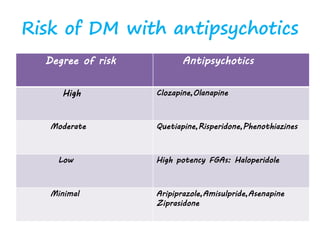
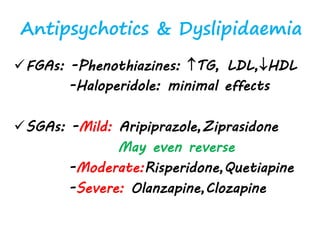
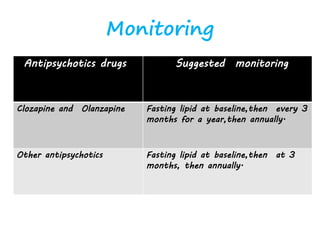
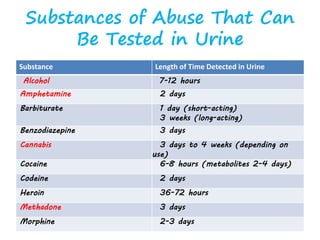
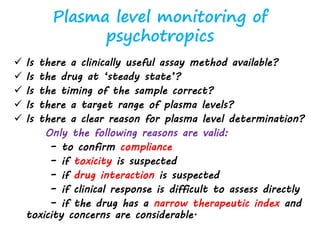
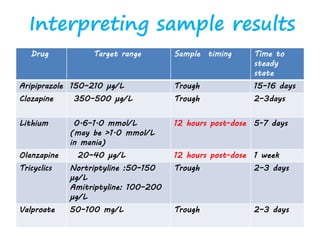
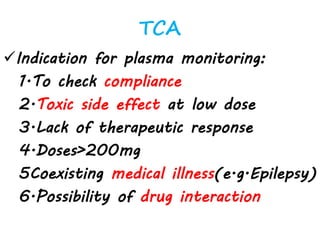
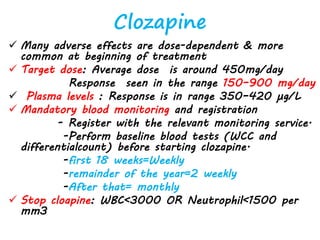
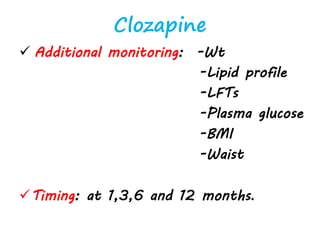
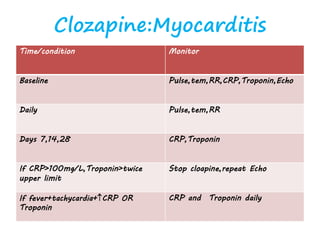
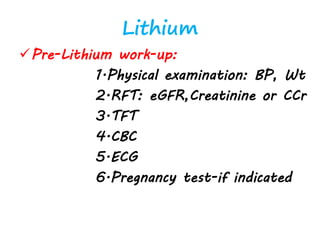
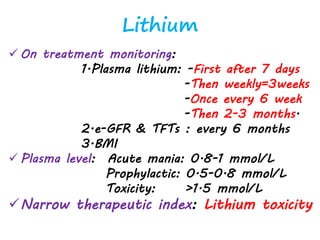
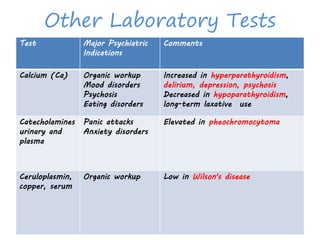
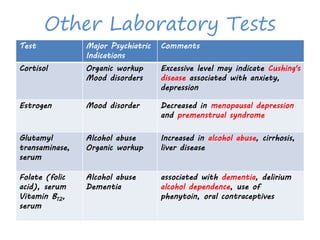
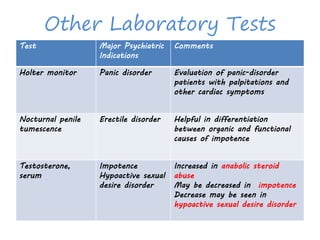
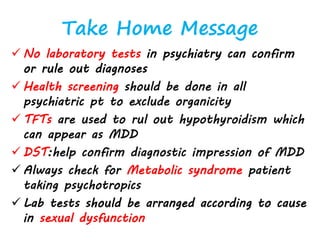
Laboratory tests play an important role in psychiatry by helping with diagnosis, monitoring treatment, and detecting potential side effects or medical comorbidities. Key tests include blood tests to evaluate thyroid, liver, kidney, and metabolic function, as well as tests for infections. Monitoring tests are important when prescribing medications like antipsychotics that can affect metabolic parameters and increase risk of conditions like diabetes. Laboratory evaluations can help optimize treatment safety and effectiveness in psychiatry.































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)





