Download to read offline

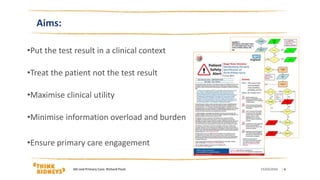
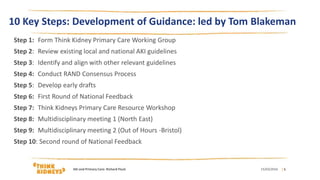
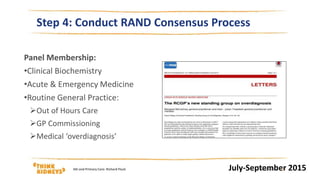
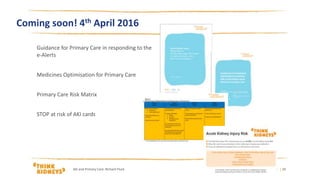

The document outlines the development of best practice guidance for primary care in responding to acute kidney injury (AKI) test results by Think Kidneys. It describes the 10 key steps taken, including forming a working group, reviewing existing guidelines, conducting a consensus process, and getting feedback. The guidance aims to put AKI test results in clinical context, treat the patient not just the test, maximize utility, and minimize burden on primary care. Forthcoming pieces include medicines optimization guidance and risk cards for primary care.