Download to read offline
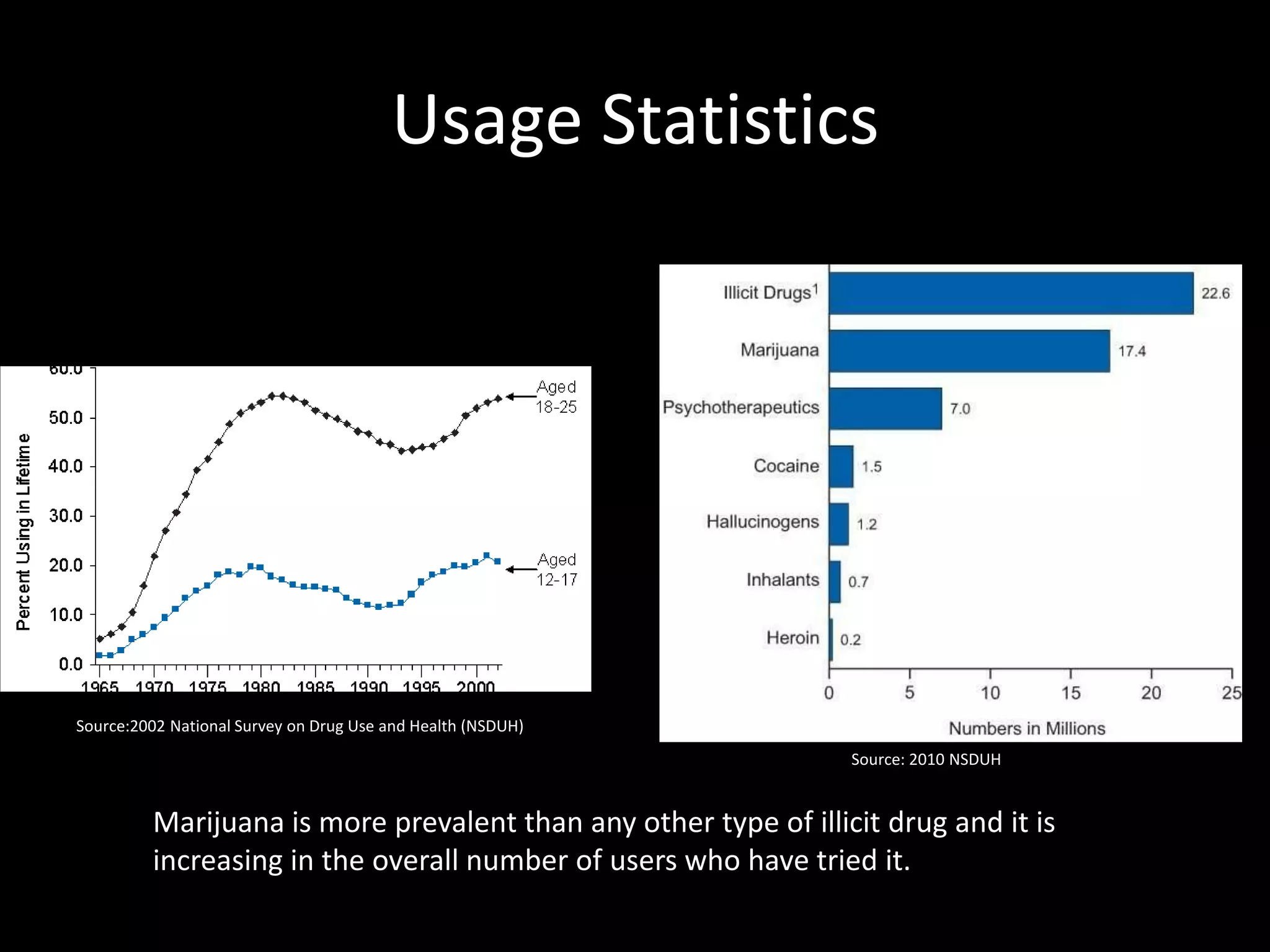
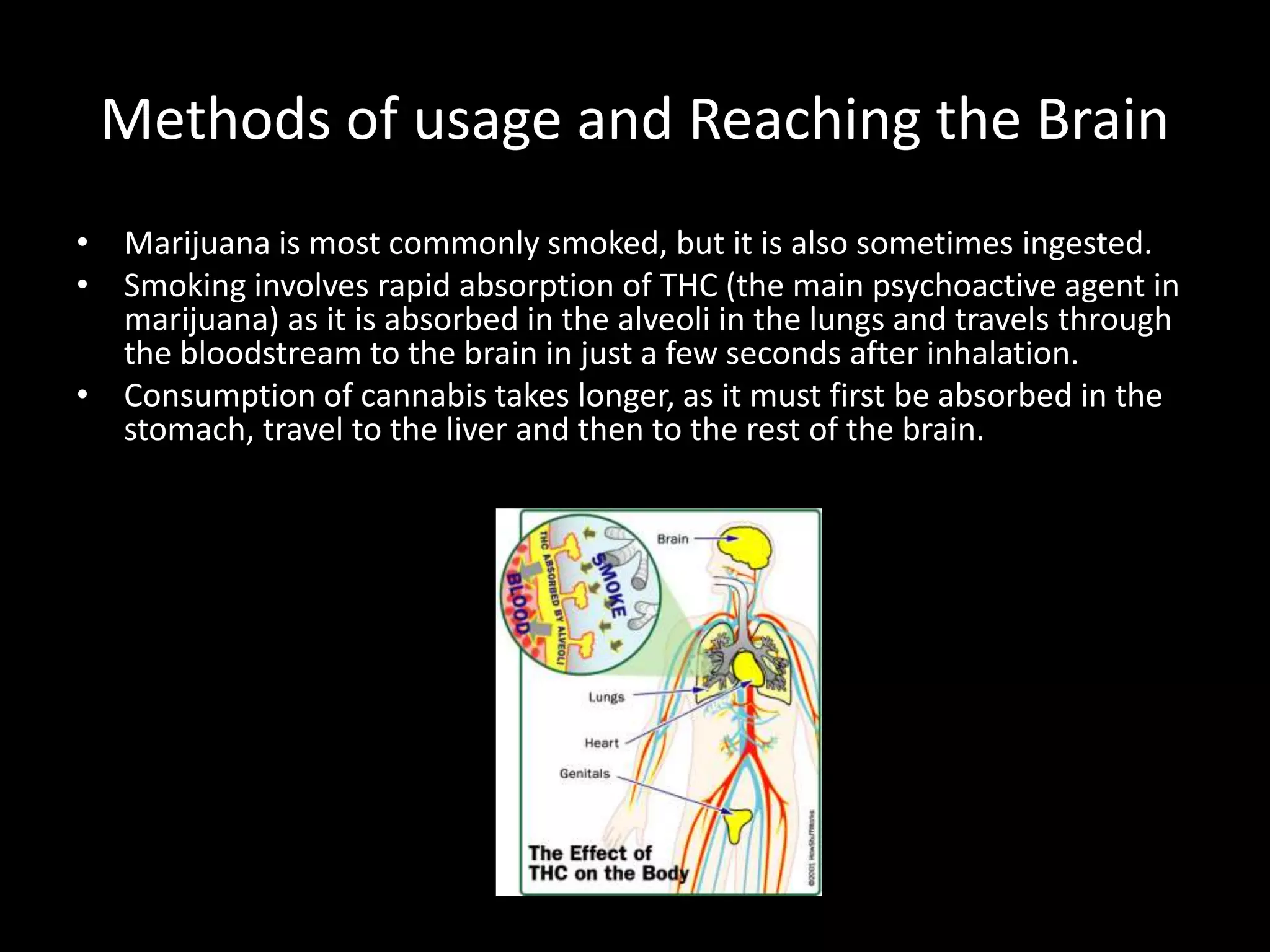
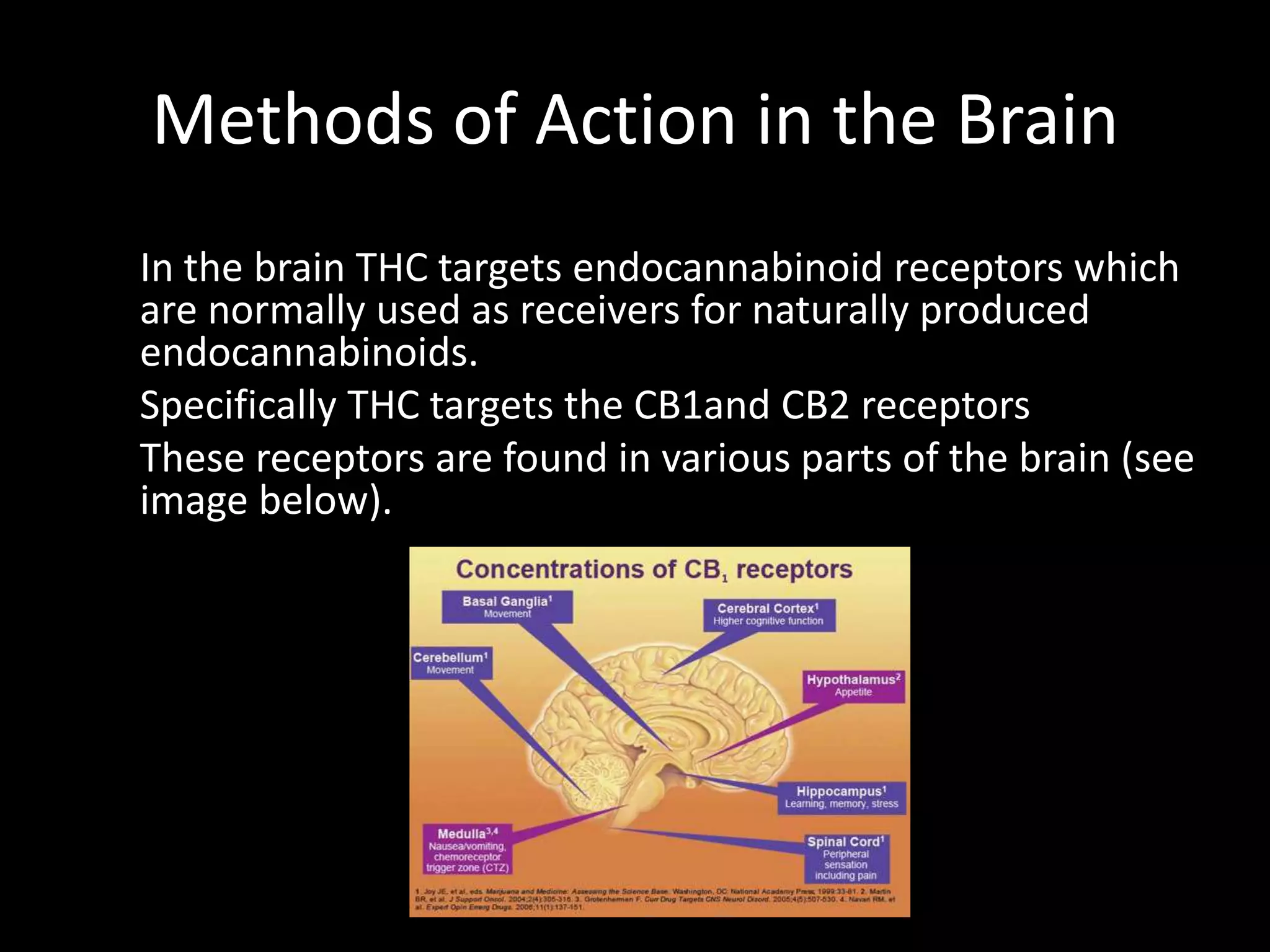
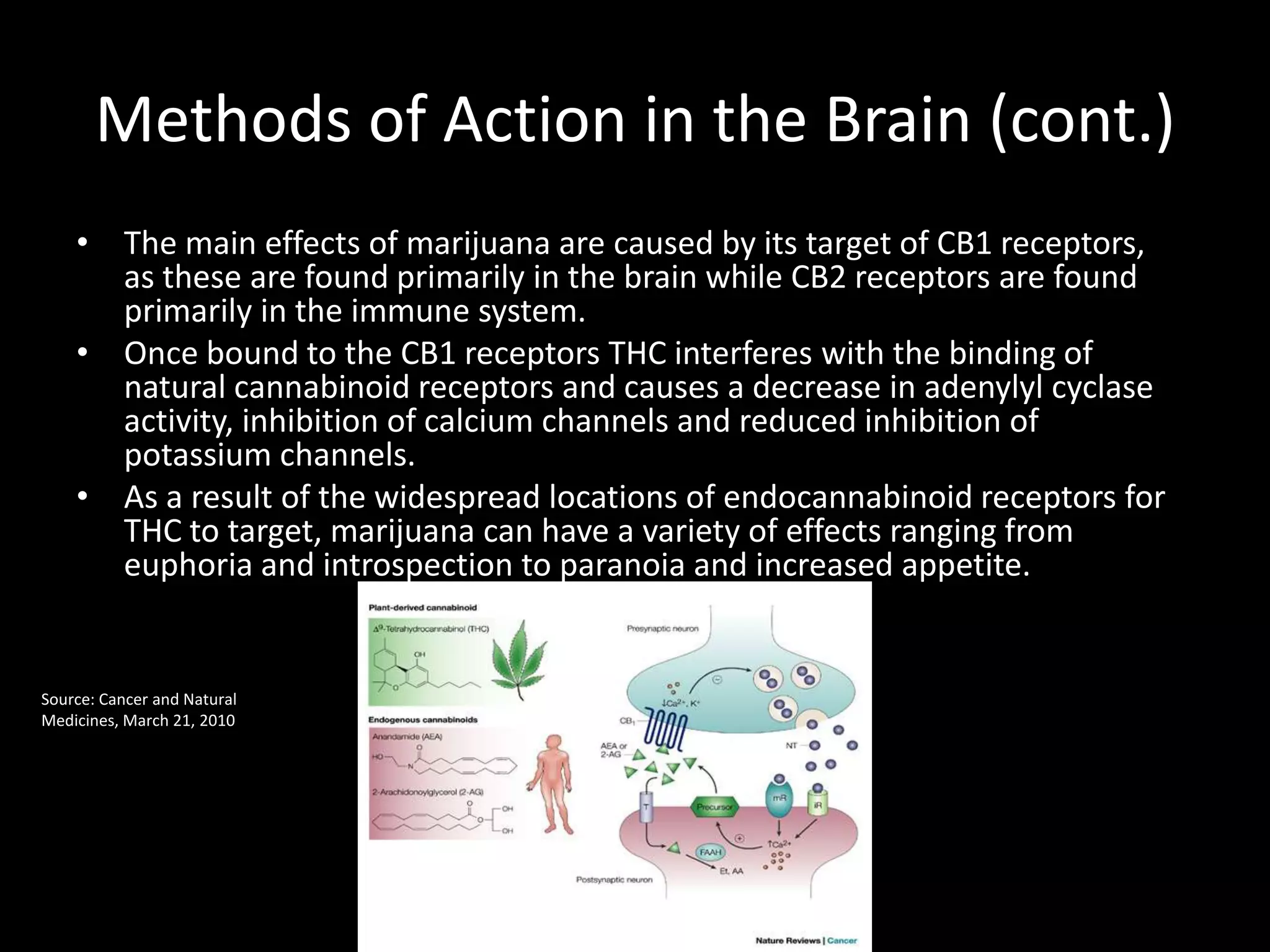

Marijuana usage is increasing, with over 50% of youth trying it. While smoking allows rapid brain absorption, consumption takes longer. THC in marijuana binds to endocannabinoid receptors in the brain, interfering with natural processes and causing varied effects. Studies on marijuana's mental health and addiction risks are mixed, but heavy usage is clearly linked to brain shrinkage and potential permanent damage. More research is still needed to fully understand marijuana's effects.






















































































