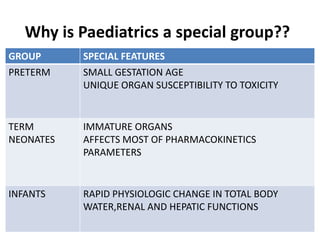
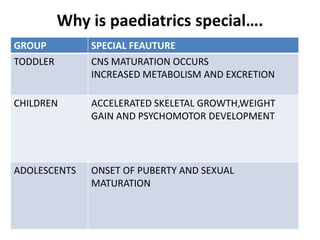
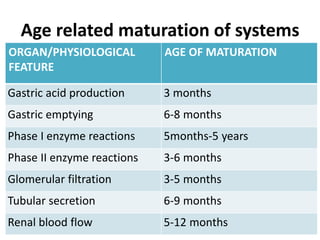
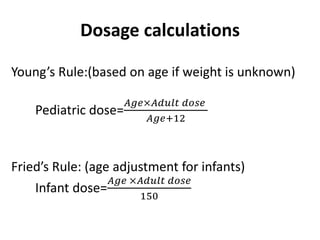
Pediatrics involves the care of infants, children, and adolescents. Knowledge of appropriate pharmacokinetics and pharmacodynamics in pediatric patients is lacking due to ethical issues in clinical trials. Dosages must account for the rapid physiological changes that occur during development, including variations in absorption, distribution, metabolism, and excretion of drugs across the different pediatric age groups. Careful dosage calculation based on body weight or surface area is necessary to ensure drug safety and efficacy in children.