Downloaded 194 times

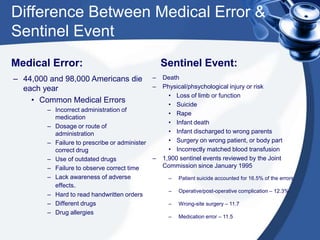


Sentinel events are unexpected occurrences involving death or serious physical or psychological injury or risk. Examples include suicide, wrong-site surgery, and infant abduction. A sentinel event differs from a medical error in its severity of outcome. Organizations are expected to report sentinel events, conduct a root cause analysis to identify causal factors, implement an action plan to reduce risks, and evaluate compliance through the survey process. The goal is to improve patient safety by learning from sentinel events.
































































