Myself Dr. Niraj N. Goswami
IInd year Resident
RIMS Raichur
Thanks to
Dr. Siddesh Kumar H Sir
Professor and HOD
RIMS Raichur
Thanks to my seniors for guidance..
Posterior uveitis
PRESENTER :DR.NIRAJ N. GOSWAMI
MODERATOR :DR. SIDDESH KUMAR H
MBBS MS FICO PEADS
PROFESSOR AND HEAD OF DEPARTMENT
DEPARTMENT OF OPHTHALMOLOGY
RIMS,RAICHUR
2.
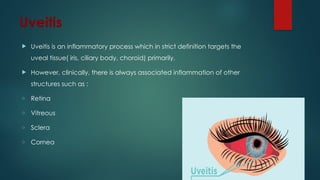
Uveitis
Uveitis isan inflammatory process which in strict definition targets the
uveal tissue( iris, ciliary body, choroid) primarily.
However, clinically, there is always associated inflammation of other
structures such as :
o Retina
o Vitreous
o Sclera
o Cornea
Clinical presentation
Thisvaries according to the location of inflammatory focus.
Peripheral lesions: Floaters
Macular lesions : Impaired central vision, metamorphopsia,
scotoma, photopsia, micropsia, macropsia
Pain, redness and photophobia are absent unless the anterior
chamber is involved.
In patients, with posterior uveitis with significant pain,
endophthalmitis or posterior scleritis should be considered.
5.
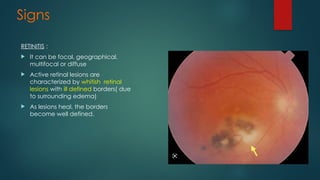
Signs
RETINITIS :
Itcan be focal, geographical,
multifocal or diffuse
Active retinal lesions are
characterized by whitish retinal
lesions with ill defined borders( due
to surrounding edema)
As lesions heal, the borders
become well defined.
7.
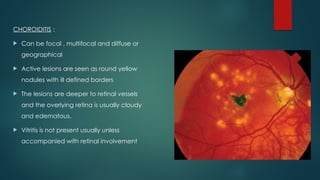
CHOROIDITIS :
Canbe focal , multifocal and diffuse or
geographical
Active lesions are seen as round yellow
nodules with ill defined borders
The lesions are deeper to retinal vessels
and the overlying retina is usually cloudy
and edematous.
Vitritis is not present usually unless
accompanied with retinal involvement
8.
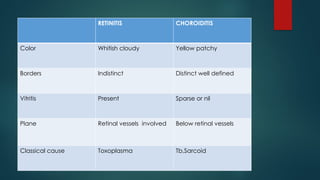
RETINITIS CHOROIDITIS
Color Whitishcloudy Yellow patchy
Borders Indistinct Distinct well defined
Vitritis Present Sparse or nil
Plane Retinal vessels involved Below retinal vessels
Classical cause Toxoplasma Tb,Sarcoid
9.
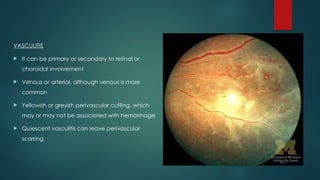
VASCULITIS
It canbe primary or secondary to retinal or
choroidal involvement
Venous or arterial, although venous is more
common
Yellowish or greyish perivascular cuffing, which
may or may not be associated with hemorrhage
Quiescent vasculitis can leave perivascular
scarring
Tuberculous Uveitis
Causativeorganism: Mycobacterium tuberculosis
Primary infection in lung which spreads via bloodstream to other
parts of the body.
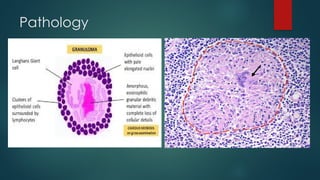
HALLMARK : Necrotising granuloma formation
In eye, TB mostly presents as uveitis (rich blood supply)
In endemic areas, it affects all age groups and cause severe
disease, whereas in non endemic areas it affects elderly people
who are immunocompromised.
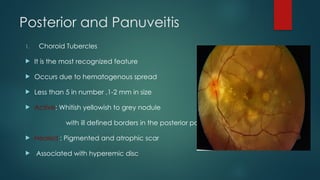
Posterior and Panuveitis
1.Choroid Tubercles
It is the most recognized feature
Occurs due to hematogenous spread
Less than 5 in number ,1-2 mm in size
Active: Whitish yellowish to grey nodule
with ill defined borders in the posterior pole
Healed : Pigmented and atrophic scar
Associated with hyperemic disc
18.
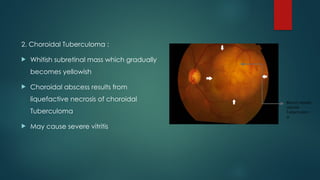
2. Choroidal Tuberculoma:
Whitish subretinal mass which gradually
becomes yellowish
Choroidal abscess results from
liquefactive necrosis of choroidal
Tuberculoma
May cause severe vitritis
Blood vessels
above
Tuberculom
a
19.
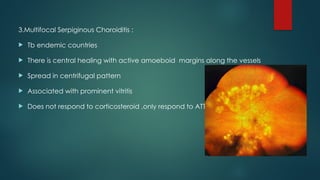
3.Multifocal Serpiginous Choroiditis:
Tb endemic countries
There is central healing with active amoeboid margins along the vessels
Spread in centrifugal pattern
Associated with prominent vitritis
Does not respond to corticosteroid ,only respond to ATT
20.
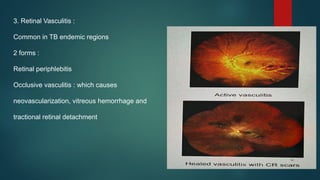
3. Retinal Vasculitis:
Common in TB endemic regions
2 forms :
Retinal periphlebitis
Occlusive vasculitis : which causes
neovascularization, vitreous hemorrhage and
tractional retinal detachment
21.
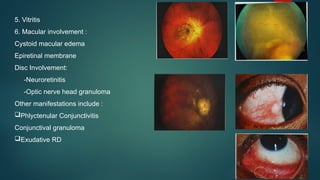
5. Vitritis
6. Macularinvolvement :
Cystoid macular edema
Epiretinal membrane
Disc Involvement:
-Neuroretinitis
-Optic nerve head granuloma
Other manifestations include :
Phlyctenular Conjunctivitis
Conjunctival granuloma
Exudative RD
22.
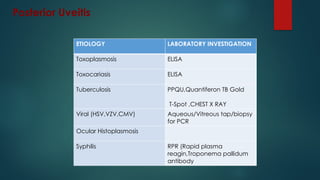
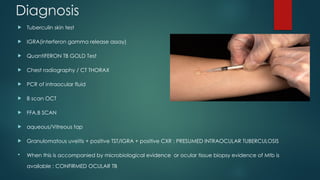
Diagnosis
Tuberculin skintest
IGRA(interferon gamma release assay)
QuantiFERON TB GOLD Test
Chest radiography / CT THORAX
PCR of intraocular fluid
B scan OCT
FFA,B SCAN
aqueous/Vitreous tap
Granulomatous uveitis + positive TST/IGRA + positive CXR : PRESUMED INTRAOCULAR TUBERCULOSIS
When this is accompanied by microbiological evidence or ocular tissue biopsy evidence of Mtb is
available : CONFIRMED OCULAR TB
Treatment
Anti TBdrug regimen :
HRZE for 2 months + HR for 4 to 7 months
Systemic Corticosteroids added to limit damage to ocular tissues
There can be paradoxical worsening after initiation of anti TB
therapy: This is managed by escalating the steroid dosage [0.5-1.0
mg/Kg] while continuing anti TB therapy.
27.
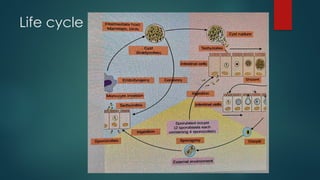
Ocular Toxoplasmosis
Causativeorganism :-
Toxoplasma gondii [Toxon-Arc Shaped]
Main cause of infectious posterior uveitis worldwide (Most common)
Obligate Intracellular parasite
Exists in three form (Depends on external conditions
-Tachyzoites
-Bradyzoites(Tissue cysts)
-Oocytes
28.
Systemic disease :
Congenitaltoxoplasmosis (2nd decade): IUD,
hydrocephalus or microcephaly, mental retardation,
intracranial calcifications etc.
Immunocompetent individuals : asymptomatic,
mononucleosis like symptoms (Fever,phyryngitis,cervical
lymphadenopathy)
Immunocompromised individuals :Reactivation of
previously inactive cyst containing scars is life threatening
complications which are mainly neurological toxoplasmic
encephalitis,retinochoroiditis
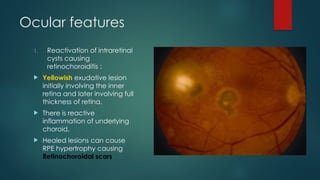
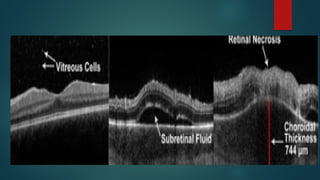
Ocular features
1. Reactivationof intraretinal
cysts causing
retinochoroiditis :
Yellowish exudative lesion
initially involving the inner
retina and later involving full
thickness of retina.
There is reactive
inflammation of underlying
choroid.
Healed lesions can cause
RPE hypertrophy causing
Retinochoroidal scars
31.
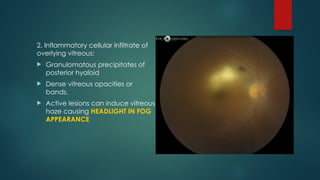
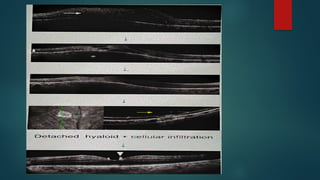
2. Inflammatory cellularinfiltrate of
overlying vitreous:
Granulomatous precipitates of
posterior hyaloid
Dense vitreous opacities or
bands.
Active lesions can induce vitreous
haze causing HEADLIGHT IN FOG
APPEARANCE
32.
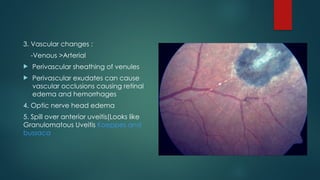
3. Vascular changes:
-Venous >Arterial
Perivascular sheathing of venules
Perivascular exudates can cause
vascular occlusions causing retinal
edema and hemorrhages
4. Optic nerve head edema
5. Spill over anterior uveitis(Looks like
Granulomatous Uveitis Koeppes and
bussaca
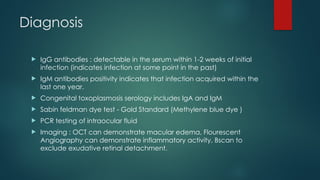
Diagnosis
IgG antibodies: detectable in the serum within 1-2 weeks of initial
infection (indicates infection at some point in the past)
IgM antibodies positivity indicates that infection acquired within the
last one year.
Congenital toxoplasmosis serology includes IgA and IgM
Sabin feldman dye test - Gold Standard (Methylene blue dye )
PCR testing of intraocular fluid
Imaging : OCT can demonstrate macular edema, Flourescent
Angiography can demonstrate inflammatory activity, Bscan to
exclude exudative retinal detachment.
37.
Treatment
Immunocompetent patients withperipheral lesions and no significant
exudation may be observed
ANTIPARASITIC DRUG + CORTICOSTEROID therapy for 5 – 6 weeks
Antiparasitic drug : Sulfadiazine + Pyrimethamine
Corticosteroid : 0.5 -1 mg/kg prednisone with tapering dose
Steroid started 24 hours after antiparasitic drug and is tapered off before it
is stopped.
Intravitreal injection of CLINDAMYCIN + DEXAMETHASONE (single or
repeated injections)
38.
In pregnancy, 10-90rule
1st trimester : Spiramycin +sulfadiazine
2nd trimester : Spiramycin+Sulfadiazine+Pyrimethamine+Folinic
acid
3rd trimester : Spiramycin+Pyrimethamine+Folinic acid
Immunosuppressed individuals and congenital toxoplasmosis are
treated regardless of the presence of retinochoroidal lesion
Standard treatment for newborn :Pyrimethamine +Sulfadiazine
+Folinic acid
39.
Cytomegalovirus Retinitis
Causativeorganism : cytomegalovirus/HHV5 (Beta Herpesviridae)
This is usually asymptomatic and manifests only in
immunocompromised individuals
It is a common opportunistic infection associated with AIDS
(CD4count<50)
It can affect affect various organs such as LUNGS, CNS, SKIN and
EYES
40.
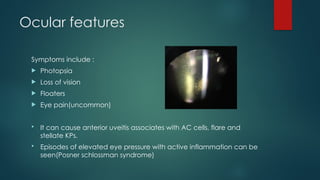
Ocular features
Symptoms include:
Photopsia
Loss of vision
Floaters
Eye pain(uncommon)
It can cause anterior uveitis associates with AC cells, flare and
stellate KPs.
Episodes of elevated eye pressure with active inflammation can be
seen(Posner schlossman syndrome)
41.
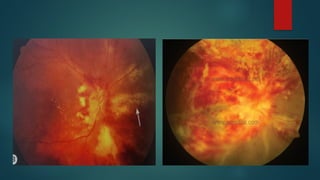
Posterior segment features
1.Retinitis and Vasculitis
Initially there is a solitary white lesion with granular borders
Associated with vasculitis which eventually causes FLAME shaped
hemorrhages (PIZZA PIE appearance)
Macular involvement causes vision loss
Initially unilateral, but later progresses to become a bilateral disease
INDOLENT FORM : peripheral granular opacities with occasional
hemorrhage
FULMINANT FORM : Vast areas of necrosis with prominent hemorrhages
along with areas of progressive retinal atrophy
43.
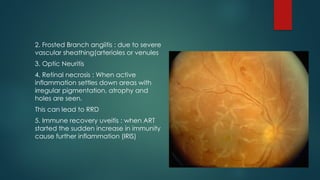
2. Frosted Branchangiitis : due to severe
vascular sheathing(arterioles or venules
3. Optic Neuritis
4. Retinal necrosis : When active
inflammation settles down areas with
irregular pigmentation, atrophy and
holes are seen.
This can lead to RRD
5. Immune recovery uveitis : when ART
started the sudden increase in immunity
cause further inflammation (IRIS)
44.
Diagnosis and Treatment
Diagnosisis mainly by PCR of ocular fluids(aqueous and vitreous)
Treatment :
Retropositive patients should be started on HAART
Systemic and intravitreal antiviral agents
VALGANCICLOVIR is the preferred agent
Induction : 900mg BD x 3 weeks
Maintenance : 900mg daily
Intravitreally : valganciclovir 2mg weekly injection(disease progression or
macula involved)
Vitrectomy with endolaser demarcation and silicone oil tamponade can be
used incase of retinal detachments
Steroids are useful in immune recovery uveitis and for frosted branch angiitis
45.
Ocular Histoplasmosis
Causativeorganism : Histoplasma capsulatum
It is a dimorphic fungus
OCULAR features :
o Multiple white atrophic chorioretinal spots
o Peripapillary atrophy
o Absent vitritis
o Choroidal neovascularization is a late feature which can cause
accumulation of subretinal fluid and hemorrhage
46.
Treatment
These patients areasymptomatic unless they develop choroidal
neovascularization in peripapillary or macular regions
Treatment involves
Intravitreal anti VEGF injection
Laser photocoagulation
Ocular photodynamic therapy with verteporfin






![Treatment
Anti TB drug regimen :
HRZE for 2 months + HR for 4 to 7 months
Systemic Corticosteroids added to limit damage to ocular tissues
There can be paradoxical worsening after initiation of anti TB
therapy: This is managed by escalating the steroid dosage [0.5-1.0
mg/Kg] while continuing anti TB therapy.](https://image.slidesharecdn.com/posterioruveitis-250530170302-527c77b2/85/Posterior-uveitis-infective-causes-for-pg-26-320.jpg)
![Ocular Toxoplasmosis
Causative organism :-
Toxoplasma gondii [Toxon-Arc Shaped]
Main cause of infectious posterior uveitis worldwide (Most common)
Obligate Intracellular parasite
Exists in three form (Depends on external conditions
-Tachyzoites
-Bradyzoites(Tissue cysts)
-Oocytes](https://image.slidesharecdn.com/posterioruveitis-250530170302-527c77b2/85/Posterior-uveitis-infective-causes-for-pg-27-320.jpg)