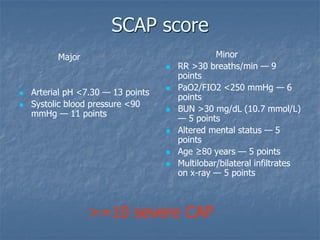
Pneumonia is an acute lung infection that can be caused by bacteria, viruses, or other pathogens. It can be diagnosed based on clinical signs and symptoms as well as tests like chest x-rays. Severity is assessed using scoring systems like CURB-65 which evaluate factors like confusion, blood urea levels, respiratory rate, blood pressure, and age. Empiric antibiotic treatment for pneumonia depends on the likely causative organisms, which vary geographically, and the patient's characteristics and severity of illness. Tests are important for confirming diagnosis and guiding targeted therapy.


























![CURB–65 score
Score one point for presence of each Clinical feature (0 –
5)
1. Confusion
2. Urea > 7 mmol/l
3. Respiratory rate 30/min
4. Blood pressure (SBP <90 or DBP 60mmHg)
5. Age 65yrs
(Albumin < 30 g/dl had an OR 4.7 [2.5-8.7] <0.001)
Lim et al Thorax 2003;58:377-382](https://image.slidesharecdn.com/pneumoniamanagement-120720033115-phpapp02/85/Pneumonia-management-30-320.jpg)