























































































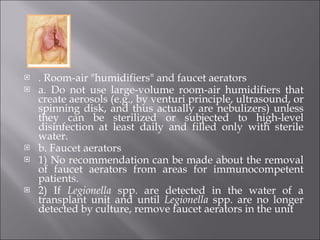
![The document also covered the prevention and control of hospital-acquired influenza and respiratory syncytial virus (RSV) infection. ] In 1994, the Healthcare Infection Control Practices Advisory Committee (HICPAC) revised and expanded the CDC Guideline for Prevention of Nosocomial Pneumonia to include Legionnaires disease and pulmonary aspergillosis.](https://image.slidesharecdn.com/pneumonia-100716224008-phpapp01/85/Pneumonia-94-320.jpg)




























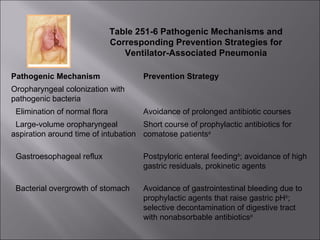
This document discusses community-acquired pneumonia (CAP), including etiology, pathogenesis, clinical presentation, diagnosis, treatment recommendations, and management based on risk stratification. Key points include: - CAP is usually caused by Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae, or Chlamydophila pneumoniae. Atypical pathogens and respiratory viruses are also common. - Clinical features may include cough, fever, tachypnea, and findings on chest exam. Chest x-ray is needed to confirm pneumonia. - Treatment depends on patient risk factors and severity, ranging from outpatient oral antibiotics for low risk to intravenous antibiotics plus macrolide for high risk or



































































































