Downloaded 50 times








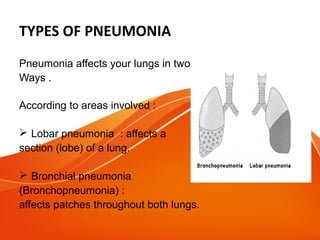



















Pneumonia is an infection of the lungs that can be caused by bacteria, viruses, or other pathogens. Common symptoms include cough, fever, shortness of breath, and chest pain. Pneumonia is usually spread through airborne droplets from coughing or sneezing. Treatment involves antibiotics if bacterial or antivirals if viral. Prevention strategies include vaccination, reducing indoor smoke and pollution, and improving nutrition and primary healthcare access.



































































