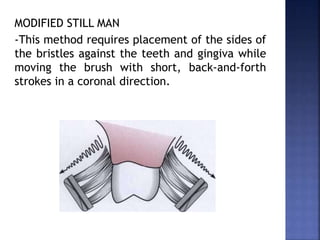
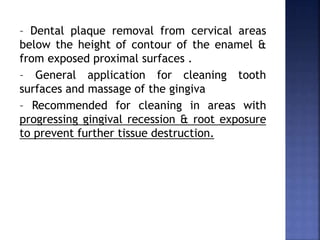
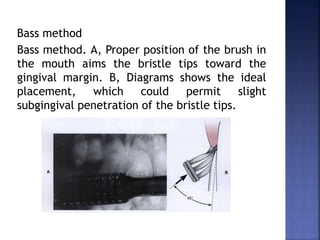
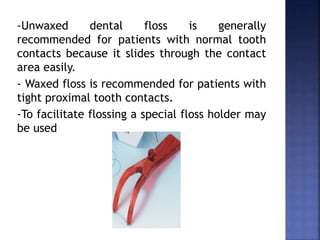
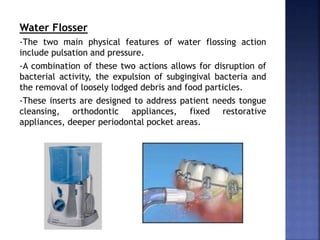
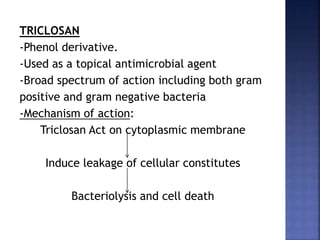
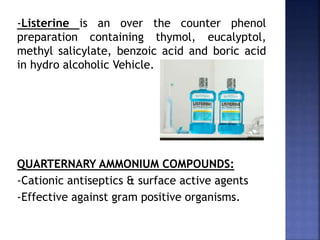
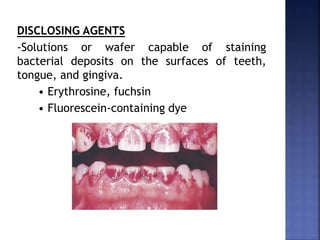
This document discusses various methods for plaque control, including mechanical and chemical approaches. Mechanical methods involve toothbrushing, flossing, and other oral hygiene aids. Proper toothbrushing techniques like Bass method and Modified Stillman are described. Chemical approaches utilize antimicrobial agents like chlorhexidine, triclosan, and povidone iodine to inhibit plaque formation. Delivery methods include toothpastes, mouthwashes, and other products. Maintaining proper plaque control is important for oral health.






















![[Crown & Bridges] [terminology & classification]](https://cdn.slidesharecdn.com/ss_thumbnails/lec01-02terminologyclassification-151105130852-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)



























![PLAQUE CONTROL.ppt [Recovered].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/plaquecontrol-220827085644-ef330fe9-thumbnail.jpg?width=640&height=640&fit=bounds)


![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


















![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)