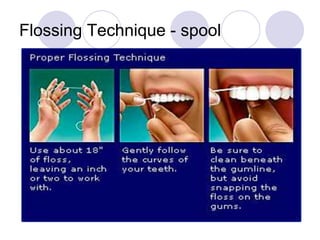
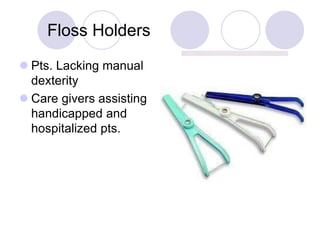
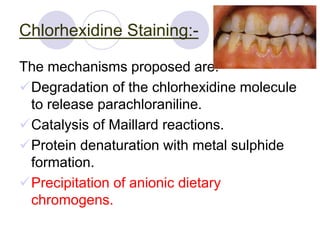
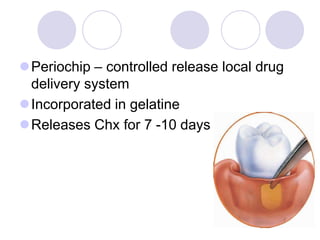
Plaque control involves both mechanical and chemical methods to remove plaque from teeth and gingiva. Mechanical methods include toothbrushing, flossing, and interdental cleaning aids. Various toothbrushing techniques like Bass, Stillman, and Charters methods are used to effectively clean different tooth and gingival areas. Powered toothbrushes provide better access and plaque removal than manual brushes. Chemical methods involve use of antimicrobial agents like chlorhexidine, triclosan, quaternary ammonium compounds, and essential oils to control plaque. Professionally delivered oral irrigation helps disrupt and remove plaque below the gumline.














































































![Plaque Control for the Periodental Patient1(1) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/plaquecontrolfortheperiodentalpatient11autosaved-251010092455-d6fc0e15-thumbnail.jpg?width=640&height=640&fit=bounds)




![PLAQUE CONTROL.ppt [Recovered].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/plaquecontrol-220827085644-ef330fe9-thumbnail.jpg?width=640&height=640&fit=bounds)





















