Sara was admitted to the labor unit with possible rupture of membranes. Upon admission, her cervix was 4 cm dilated, -3 station, and 80% effaced. She was experiencing regular contractions.
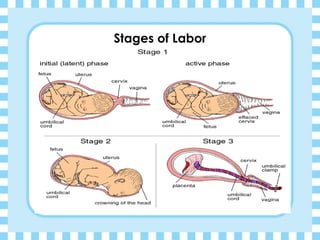
The document provides information on the stages of labor, including the three stages of the first stage (latent, active, transition), signs of each stage, and nursing care required. It also discusses factors that can influence the duration of labor like fetal position and size, as well as maternal health factors.
Nursing diagnoses for Sara's admission include risks for injury, pain, fear, and infection due to her status on admission and the labor process. Proper monitoring, fluid management, and communication are important for





















![Normal labour [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/normallabourautosaved-200123025541-thumbnail.jpg?width=640&height=640&fit=bounds)


























