Downloaded 76 times




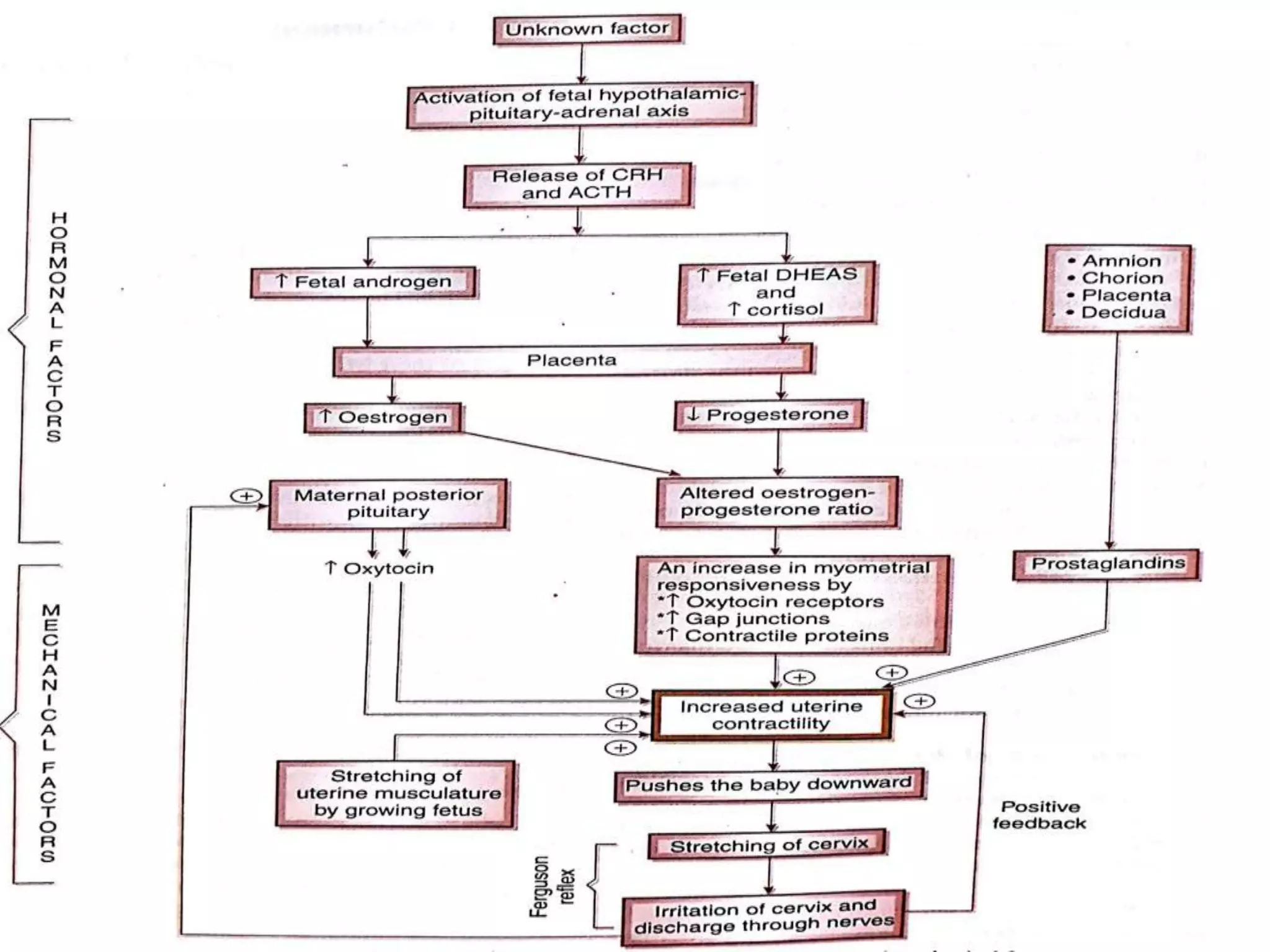







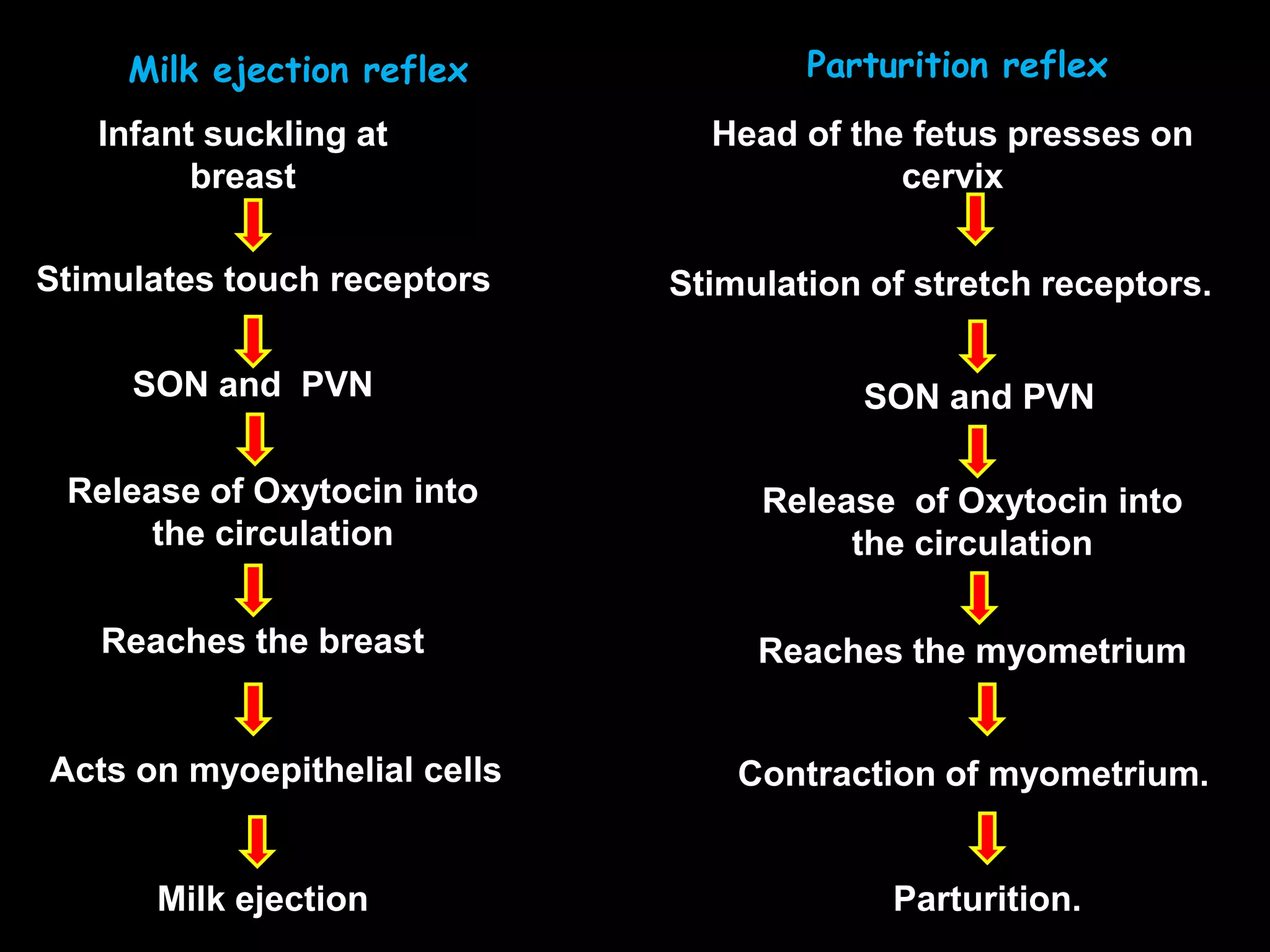



The document summarizes the physiology of parturition (childbirth) and lactation. It describes the four stages of labor, including cervical dilation and effacement in the first stage and delivery of the baby in the second. It discusses the hormonal and mechanical factors that control parturition, such as increased estrogen and progesterone levels triggering uterine contractions. The document also explains lactogenesis, including the hormonal influences of prolactin, progesterone, estrogen and oxytocin in milk production and ejection.






















































































