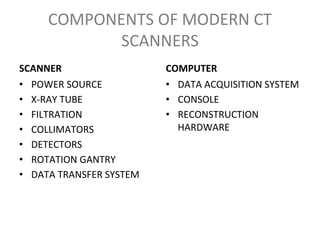
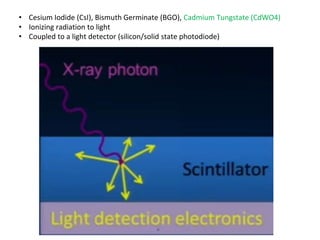
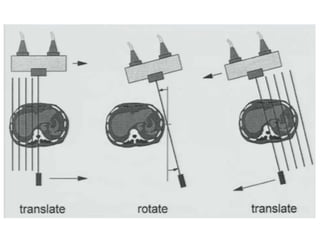
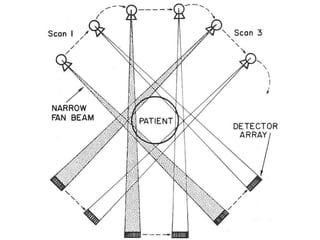
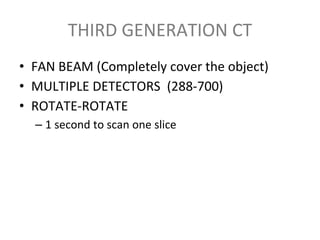
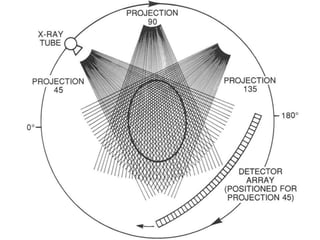
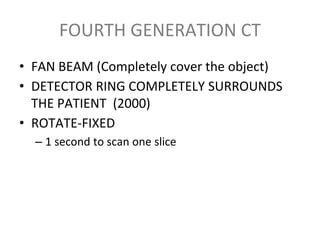
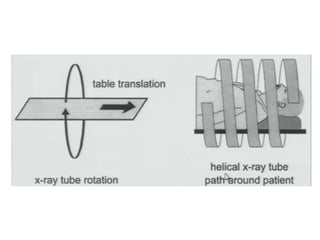
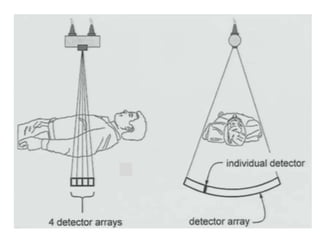
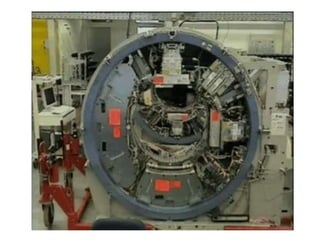
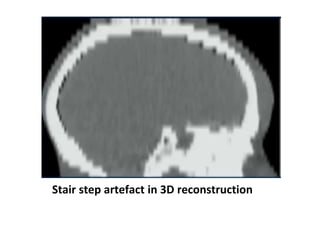
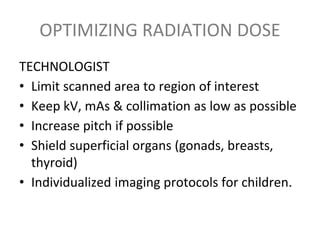
The document discusses the components and evolution of computed tomography (CT) scanners. It describes the basic principles of CT imaging and how CT scanners have progressed from early generations with single detectors and pencil beams to current multi-detector systems that can acquire multiple slices simultaneously in under one second. It also summarizes key factors that influence image quality such as spatial resolution, noise, and radiation dose, as well as common artifacts and techniques for dose optimization.