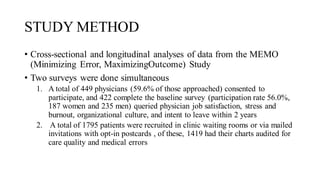
This document summarizes three journal club presentations on physician burnout. The first presentation defines burnout and its components, and reviews a study that found higher burnout among interns and residents in certain specialties. The second presentation reviews a study finding associations between long work hours, burnout, and medical errors among Chinese physicians. The third presentation summarizes a study finding that women primary care physicians and those with less work control reported more burnout, and burned out physicians were less satisfied and more likely to report errors.


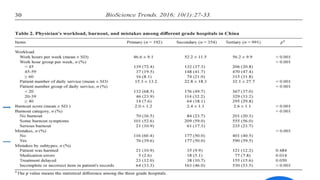
![RESULT
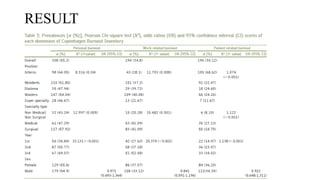
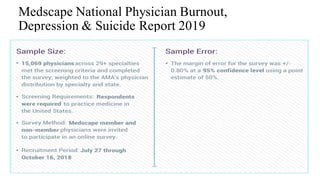
• A total of 4355 of 6490 (67%) respondents were male,
• with a median age of 56 (interquartile range [IQR], 45-63) years,
• median of 50 hours worked per week, and a median of 1 nights on call per week](https://image.slidesharecdn.com/physicianburnout-200717214331/85/Physician-burnout-42-320.jpg)
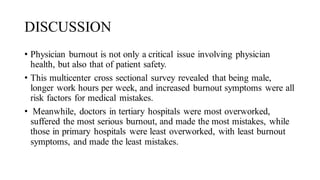
![Conti…
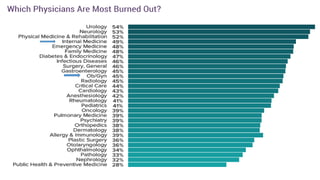
• Of 6586 respondents, 691 (10.5%) reported a self-perceived major medical error
in the previous 3 months
• Errors were most commonly categorized as an
• error in judgment (266 of 679 respondents[39.2%]),
• wrong diagnosis (136 of 679 [20.0%]), or
• technical mistake (88 of 679 [13.0%])](https://image.slidesharecdn.com/physicianburnout-200717214331/85/Physician-burnout-43-320.jpg)
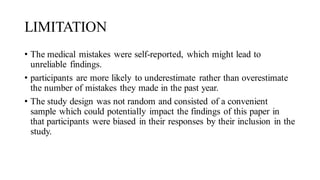
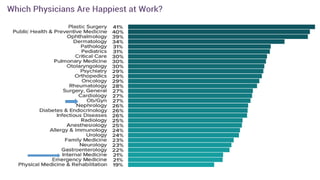
![• The highest prevalence of medical errors was reported
by respondentsfrom radiology (58 of 249 respondents
[23.3%]), neurosurgery (12 of 55 [21.8%]), and
emergency medicine (74 of 346 [21.4%])
• More than half of all errors (367 of 663 respondents
[55.4%])had no perceived effect on patient outcome,
but 35 (5.3%) resulted in “significant permanent
morbidity” and 30 (4.5%) in a patient death](https://image.slidesharecdn.com/physicianburnout-200717214331/85/Physician-burnout-44-320.jpg)






























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




